Zygomatic Dental ImplantsFixed Teeth When the Upper Jaw Has Run Out of Bone
- Zygomatic dental implants exist because conventional implant dentistry, including the All-on-4 graftless protocol, runs out of bone before some patients run out of options.
When severe maxillary atrophy leaves the upper jaw with insufficient bone for any standard implant placement, zygomatic implants bypass the jaw entirely: they travel through the maxillary sinus and anchor in the zygomatic bone, the cheekbone, which maintains density regardless of how much alveolar ridge has resorbed.
Overview
Zygomatic dental implants exist because conventional implant dentistry, including the All-on-4 graftless protocol, runs out of bone before some patients run out of options. When severe maxillary atrophy leaves the upper jaw with insufficient bone for any standard implant placement, zygomatic implants bypass the jaw entirely: they travel through the maxillary sinus and anchor in the zygomatic bone, the cheekbone, which maintains density regardless of how much alveolar ridge has resorbed.
Zygomatic implants demonstrated 10-year cumulative survival rates of 96.7% in a multi-centre study of 556 implants, with same-day loading achieved in 94.3% of cases. No significant difference in survival was observed between quad-zygomatic and hybrid zygomatic-standard configurations.
At Stunning Dentistry, we perform zygomatic implant surgery with surgeons who hold specific zygomatic certification and documented case volume. Candidacy is evaluated by CBCT analysis of both the residual maxillary bone and the zygomatic arch geometry. Same-day loading is gated by the same SD-TIAD-02 criteria applied to All-on-4 cases, plus additional sinus health screening.
Questions about this procedure?
What Are Zygomatic Implants?
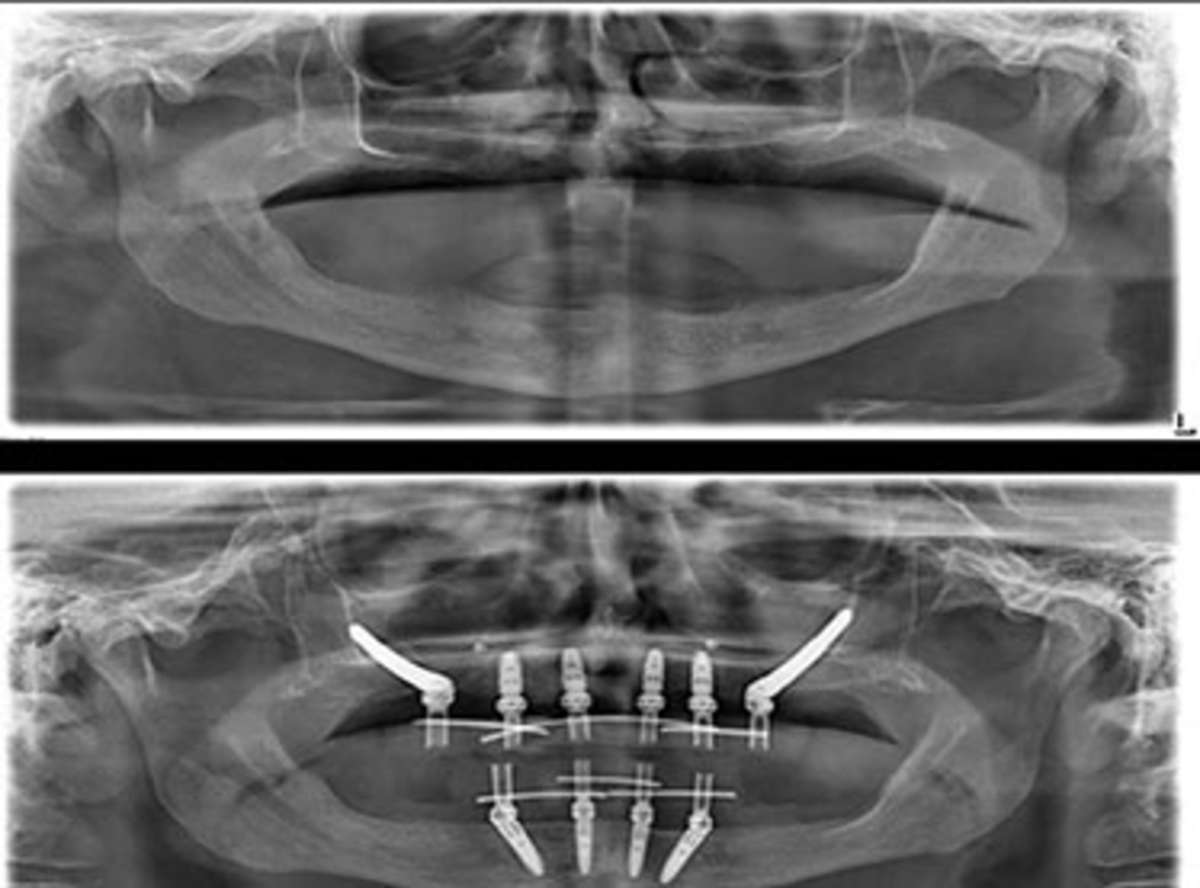
Zygomatic implants are long-body titanium fixtures (typically 30–52.5 mm) that originate at or near the alveolar crest, traverse the maxillary sinus, and achieve primary anchorage in the cortical bone of the zygomatic arch. Two zygomatic implants, one on each side, can anchor a full-arch maxillary prosthesis. When bone allows, two standard anterior implants are added for additional anterior support (hybrid configuration). When no anterior alveolar bone exists, quad-zygomatic (four zygomatic implants, two on each side) provides full-arch support without any standard implants.
The zygomatic bone provides dense cortical anchorage independent of alveolar bone volume. In patients with Cawood & Howell Class V–VI maxillary atrophy, zygomatic implants provide the only implant-based solution without bone augmentation.
At Stunning Dentistry, we review every zygomatic implant case with the full surgical and prosthodontic team before the treatment plan is finalised. Zygomatic implants are not a product, they are a surgical solution for a specific and severe anatomical problem, and they are recommended only when the anatomy requires them.
Ready to discuss your options?

Why the Zygoma?
The maxillary alveolar ridge loses bone progressively after tooth loss, a process driven by absence of masticatory stimulation, accelerated by periodontal disease, and sometimes catastrophically worsened by failed implant attempts or previous denture compression. After years of resorption, the ridge may be too thin, too short, or too pneumatised by sinus expansion to place any standard implant. Bone grafting can reconstruct this ridge, but the process takes 9–18 months, requires a graft source (hip, chin, or synthetic material), and still may not produce bone of adequate volume in severely atrophied patients.
In Cawood and Howell Class V–VI maxillary atrophy, bone grafting achieves implant-compatible bone volume in only 67% of cases, with a 24% complication rate and a mean 14-month augmentation period before implant placement.
At Stunning Dentistry, we base the choice between zygomatic implants and bone grafting + conventional implants on CBCT measurement. If your residual bone is sufficient for conventional implants, even with grafting, we will tell you. If zygomatic implants are the only viable path to a fixed arch without augmentation, we will explain the anatomy on your scan and document why.
Curious about costs and timelines?

Long-Term Survival Data
The pooled 95.2% survival across the largest systematic review, spanning up to 10 years, is the most important number for patient decision-making: zygomatic implants do not have inferior long-term outcomes compared with standard implants in equivalent patients. The difference is that the patients treated with zygomatic implants had no standard implant option. These are outcomes in the most anatomically challenging cases in implant dentistry.
| Study / Source | Follow-Up | Implant Count | Survival Rate | Notes |
|---|---|---|---|---|
| Aparicio et al. (2021) | 10 years | 556 implants | 96.7% | Multi-centre, hybrid + quad configurations |
| Davó R et al. (2018) | 5 years | 344 implants | 97.4% | Immediate loading, quad-zygomatic |
| Malo et al. (2015) | 3 years | 188 implants | 98.2% | Hybrid zygomatic + standard |
| Bothur & Garsten (2010) | 10 years | 40 patients | 94.9% | Single-centre, long-term follow-up |
| Chrcanovic & Abreu Albrektsson (2013) systematic review | 1–10 years | 2,402 implants | 95.2% (pooled) | Largest systematic review to date |
Want a personalised treatment plan?
Who Is a Candidate?
Zygomatic implants are indicated for patients with severe maxillary atrophy who either: (a) do not have adequate alveolar bone for All-on-4 standard or tilted implants; (b) have failed previous bone grafting attempts; or (c) require a solution without the 12–18 month augmentation timeline. They are exclusively a maxillary (upper jaw) procedure, the mandible does not have equivalent anatomy.
Zygomatic implants are indicated for patients with Cawood and Howell Class IV, V, or VI maxillary atrophy, and for patients in whom previous augmentation has failed or is contraindicated by systemic factors.
At Stunning Dentistry, we require sinus health screening as mandatory pre-surgical clearance for every zygomatic case. Active sinusitis, significant sinus pathology, or nasal polyps require ENT clearance before proceeding. These are not disqualifiers, they are conditions that must be managed before zygomatic surgery is safe.
Questions about this procedure?
Graftless Immediate-Loading Protocol
The zygomatic implant's anchorage in dense cortical cheekbone typically achieves insertion torque values significantly higher than standard implants in atrophic maxillary bone, often exceeding 50–70 Ncm. This high primary stability is what makes same-day loading consistently achievable in zygomatic cases, even in patients whose alveolar bone was completely inadequate for any implant placement.
Immediately loaded zygomatic implants achieved 94.3% same-day loading rate in a 556-implant multi-centre cohort, with implant survival equivalent to delayed-load controls at 5-year follow-up.
At Stunning Dentistry, we apply the SD-TIAD-02 gate protocol to zygomatic cases with modifications: the sinus health gate (pre-surgical ENT screening) and sinus membrane integrity (assessed intra-operatively) are added to the standard seven-gate battery. Immediate loading proceeds only when all gates pass.
Ready to discuss your options?
Benefits
Zygomatic implants deliver what no other protocol can for severely atrophic maxillary patients: fixed teeth without bone grafting, without an 18-month augmentation timeline, and often with same-day function. For patients who have spent years in removable dentures that no longer fit, because the underlying ridge has resorbed to the point where suction retention fails, zygomatic implants end that period in a single surgical event.
Quality of life scores (OHIP-14) in zygomatic implant patients showed the largest gains of any implant rehabilitation group at 12 months, a finding consistent with the fact that these patients had the most severe pre-treatment functional compromise.
At Stunning Dentistry, zygomatic implant cases are presented with full pre-surgical imaging, surgical plan, and outcome expectations discussed in your consultation. The benefit we explain is anatomical and functional, not aspirational.
Curious about costs and timelines?

Recovery Timeline
Swelling after zygomatic implant surgery is more pronounced than after standard implant procedures, the surgical corridor traverses soft tissue, sinus membrane, and the lateral wall of the maxilla. Patients typically experience moderate facial swelling for 10–14 days. This is a normal healing response to the surgical anatomy, not a complication indicator.
| Phase | Timeframe | What Happens | Your Responsibility |
|---|---|---|---|
| Surgical Day | Day 0 | Zygomatic implants placed, provisional fixed (if gates pass) | Accompanied transport, no driving |
| Acute Healing | Days 1–10 | Significant swelling, more than standard implants (cheekbone surgery) | Ice, head elevation, liquid to soft diet |
| Sinus Drainage Period | Days 3–7 | Some nasal discharge is normal, sinus was traversed | Prescribed nasal rinse, no blowing nose forcefully |
| Early Integration | Weeks 2–12 | Osseointegration in zygomatic cortex | Soft diet strictly maintained |
| Provisional Review | Week 10–12 | ISQ measured at all implants, sinus health checked | Attend review |
| Definitive Impressions | Months 4–5 | Digital or physical impressions for definitive prosthesis | Attend all impression appointments |
| Definitive Fit | Months 5–7 | Definitive monolithic zirconia fitted | Attend fit appointment |
| 12-Month Review | Month 12 | CBCT or periapical review, sinus health assessed, bone levels | Attend review |
Want a personalised treatment plan?

Complications
The most procedure-specific complication of zygomatic implants is sinusitis, occurring in approximately 5–10% of cases in published series. The implant traverses the maxillary sinus, and the sinus membrane is elevated or penetrated during the procedure. In most cases the sinus adapts without event. In some cases, chronic sinusitis develops around the implant exit point, requiring antibiotic management, sinus irrigation, or in rare cases endoscopic sinus surgery.
Sinusitis was the most procedure-specific complication in zygomatic implant cases, with a cumulative incidence of 8.9% at 5 years, predominantly in cases with pre-existing sinus pathology or sinus membrane perforation without membrane repair.
At Stunning Dentistry, pre-surgical ENT assessment is mandatory for zygomatic cases. Sinus health is not assumed, it is documented. Post-operatively, all zygomatic patients receive a nasal rinse protocol, saline irrigation guidance, and a written instruction for their Canadian GP on when to suspect sinus complications.
Questions about this procedure?
Comparison Table
| Factor | Zygomatic Implants | All-on-4 | Bone Graft + Convention Implants | Overdenture |
|---|---|---|---|---|
| Bone requirement | Severe atrophy, no maxillary bone needed | Moderate anterior bone | Any, augmented | Minimal |
| Bone grafting | Never | Rarely | Always | Rarely |
| Anchorage site | Zygomatic arch (cheekbone) | Alveolar bone (jaw) | Augmented alveolar bone | Alveolar bone |
| Immediate loading | Yes (gated, high success rate) | Yes (gated) | Usually delayed | Usually yes |
| Prosthesis type | Fixed | Fixed | Fixed | Removable |
| Sinus involvement | Yes, traversal required | Avoided (tilted design) | Often involved (sinus lift) | No |
| Timeline to definitive | 5–7 months | 4–6 months | 14–24 months | 2–3 months |
| CAD Cost (Stunning Dentistry) | $22,000–$32,000/arch | $14,000–$20,000/arch | $25,000–$40,000/arch | $8,000–$12,000/arch |
| CAD Cost (Canada private) | $70,000–$100,000 | $45,000–$65,000 | $60,000–$90,000 | $20,000–$35,000 |
Ready to discuss your options?

Cost Factors
Stunning Dentistry CAD range: $22,000–$32,000 per arch (all-inclusive)
Canadian public system: Not available for elective implant treatment
| Cost Factor | Lower Range | Higher Range | Driver |
|---|---|---|---|
| Configuration | Hybrid (2 zygomatic + 2 standard) | Quad-zygomatic (4 zygomatic) | Number of zygomatic implants |
| Implant system | Straumann ZAGA / Nobel Biocare Zygoma | Zimmer Biomet Zygoma | System selection, surgeon preference |
| Prosthesis material | Hybrid metal-acrylic | Monolithic 5Y-TZP zirconia | Material cost, milling |
| Surgical complexity | Standard zygomatic anatomy | Complex sinus anatomy, prior failed grafts | Surgical time, added instrumentation |
| Sedation | Local + IV | General anaesthesia | Anaesthetic complexity |
Curious about costs and timelines?

Step-by-Step
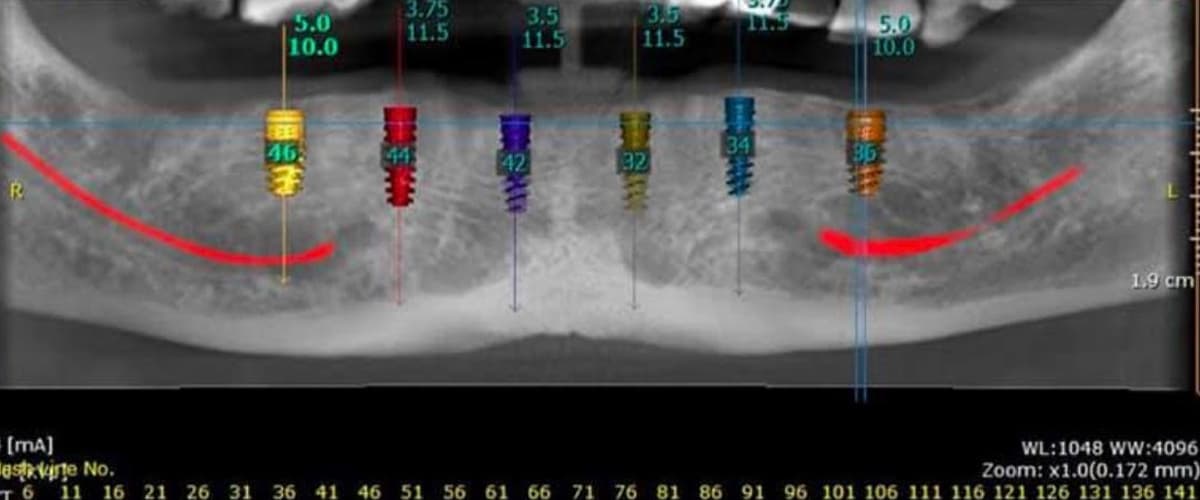
Day 1, CBCT and Zygomatic Planning: Cone-beam CT with dedicated zygomatic software analysis. The implant pathway through the sinus to the zygomatic arch is planned digitally. Sinus health assessed. ENT clearance confirmed if any sinus pathology detected.
Day 2–3, Extractions (if required): Any remaining maxillary teeth are extracted. Soft tissue allowed to heal sufficiently for prosthetic-level planning.
Day 3–5, Zygomatic Implant Surgery: Under local anaesthesia with IV sedation or general anaesthesia. The zygomatic surgical corridor is opened via a crestal or palatal incision. The maxillary sinus lateral wall is fenestrated. The implant is guided through the sinus and into the zygomatic arch under direct vision or endoscopic assistance. Insertion torque measured. ISQ measured with Osstell. Standard anterior implants placed if hybrid configuration.
Gate Assessment and Loading Decision: If all SD-TIAD-02 gates pass including sinus integrity check, provisional fitting proceeds.
Provisional Fitting: Fixed provisional fitted to all implants (zygomatic + standard if present). Occlusion load-protected. Patient discharged with nasal rinse protocol and soft diet instructions.
Week 10–12 Review: ISQ measurements, sinus health assessment, occlusion check. Definitive impressions if integration confirmed.
Month 5–7, Definitive Delivery: Definitive monolithic zirconia prosthesis fitted and torque-locked. Written aftercare and Dental Angel handover documentation provided.
Want a personalised treatment plan?

Aftercare
Zygomatic implant aftercare includes both the standard implant hygiene protocol and an additional sinus health monitoring component. The sinus traversal means that nasal symptoms, post-nasal drip, intermittent pressure, minor congestion, may persist for 3–6 months as the sinus membrane adapts to the implant passage. This is expected, documented, and does not indicate a complication unless accompanied by frank sinusitis symptoms (purulent discharge, pain, fever).
Patients who reported chronic nasal symptoms after zygomatic implant surgery without clinical signs of sinusitis experienced symptom resolution in 89% of cases within 6 months, without surgical intervention.
At Stunning Dentistry, your Dental Angel handover document for zygomatic cases includes a GP letter explaining that you have had zygomatic implants placed, what sinus traversal means clinically, and what symptoms warrant ENT referral. Your Canadian GP is not managing an undocumented case.
Questions about this procedure?
Aftercare Responsibility Split
| Task | Timeframe | Who | How |
|---|---|---|---|
| Nasal saline rinse | First 4–6 weeks post-surgery | Patient | Neil Med sinus rinse or equivalent, 2× daily |
| Avoid nose-blowing with force | First 3 weeks | Patient | Gentle nose blowing only, no sneezing with mouth closed |
| Soft diet compliance | First 10–12 weeks | Patient | Soft-cooked foods, no hard or crunchy items |
| Daily interdental brush | From Week 2 | Patient | 1.0–1.5 mm at each abutment site |
| Water flosser irrigation | From Week 2 | Patient | Medium pressure, all gingival margins |
| 48-hour check-in | Day 2 | Stunning Dentistry | Phone or video review |
| Sinus symptom monitoring | Ongoing | Patient + Stunning Dentistry | Report nasal symptoms lasting >3 weeks |
| Professional ultrasonic cleaning | Every 6 months | Home dentist | Subgingival access at all abutments |
| Annual sinus health assessment | Annually | Canadian GP or ENT | Clinical or radiographic review |
| Annual bone level X-rays | Annually | Home dentist | Periapical at all implant abutment sites |
Ready to discuss your options?
When Zygomatic Implants Are Not Recommended
Zygomatic implants are a solution for a specific anatomical problem, severe maxillary atrophy, and are contraindicated when that problem does not exist or when sinus health cannot support the surgical approach. They are a more anatomically complex procedure than All-on-4 and should not be selected when conventional implants, with or without bone grafting, are viable. More surgery is not better surgery when less surgery achieves the same outcome.
Zygomatic implants should be reserved for patients with Cawood and Howell Class IV–VI maxillary atrophy where conventional implant placement is not feasible with or without bone augmentation. Using zygomatic implants in patients with adequate alveolar bone increases procedural complexity without clinical benefit.
At Stunning Dentistry, we recommend zygomatic implants only when CBCT confirms that conventional implant placement, including grafting, is not viable or not preferred by the patient. We will not recommend a more complex surgical pathway when a simpler one exists. If your anatomy allows conventional arch rehabilitation, that is what we recommend.
| Contraindication | Type | Path Forward |
|---|---|---|
| Adequate alveolar bone for conventional implants | Absolute for zygomatic | All-on-4 or All-on-6 recommended |
| Active sinusitis or rhinosinusitis | Absolute until cleared | ENT treatment, then re-evaluate |
| Nasal polyps or chronic sinus pathology | Absolute until cleared | ENT surgical clearance required |
| Immunosuppression (active) | Absolute | Prescriber consultation; defer |
| Anticoagulation (unmanageable perioperatively) | Absolute | Haematology consultation required |
| Severe trismus limiting surgical access | Relative | Physiotherapy; reassess access |
| Intra-operative sinus membrane perforation | Surgeon decision to manage or defer | ENT referral if significant |
Curious about costs and timelines?
Myths vs Reality
"Zygomatic implants are experimental."
Zygomatic implants require specific surgical training, dedicated instrumentation, and documented case experience. The risk profile of the procedure, sinus traversal, proximity to the orbital floor, extended implant pathway, is categorically different from standard implantology. Surgeon credentials and case volume are the most important clinical safety factors to verify.
Want a personalised treatment plan?
People Also Ask
What are zygomatic implants and who needs them?
Zygomatic implants are long titanium fixtures anchored in the cheekbone (zygomatic arch) to support a full upper-arch prosthesis in patients with severe jaw bone loss.
They are indicated for patients with Cawood and Howell Class IV–VI maxillary atrophy, patients who have lost so much upper jaw bone that conventional or All-on-4 implants are not possible without extensive grafting.
Canadian oral surgeon and prosthodontist combined fees for zygomatic implants range from CAD $70,000–$100,000.
Stunning Dentistry's all-inclusive fee is CAD $22,000–$32,000 per arch in India, using the same Straumann ZAGA or Nobel Biocare zygomatic implant systems.
The largest systematic review of 2,402 zygomatic implants showed a pooled 10-year survival rate of 95.2%.
A multi-centre study of 556 implants showed 96.7% survival at 10 years. Long-term outcomes are comparable to standard implants in equivalent anatomical difficulty patients.
Same-day loading was achieved in 94.3% of cases in a large multi-centre study.
The cheekbone consistently provides high primary stability (often >50 Ncm insertion torque), which supports immediate loading in most cases. The SD-TIAD-02 protocol gates the decision intra-operatively.
Is zygomatic implant surgery dangerous?
Zygomatic implant surgery is a specialist procedure with a defined risk profile including approximately 8–10% sinusitis rate and rare orbital complications when performed outside protocol.
When performed by a zygomatic-trained surgeon under documented protocol by a team with adequate case volume, the complication profile is acceptable and the procedure is the standard of care for its indication.
Questions about this procedure?
Ask Your Doctor
1. What is my CBCT Cawood and Howell classification and what does it indicate about the zygomatic vs standard implant decision?
2. What is the planned implant configuration, hybrid (zygomatic + standard) or quad-zygomatic?
3. What is the planned pathway of the zygomatic implants through my sinus anatomy specifically?
4. Does my sinus health require ENT clearance before surgery?
5. What is your zygomatic implant case volume and what training have you completed?
6. What insertion torque do you expect to achieve and what is the loading threshold?
7. What is the written warranty on the zygomatic implants and the prosthesis?
8. What sinus complications have you encountered in your zygomatic cases and how were they managed?
9. How will my Canadian GP and dentist be briefed on my case, including the sinus component?
10. What nasal or sinus symptoms after returning to Canada should prompt me to contact you?
Ready to discuss your options?

For Canadian Patients
For Canadian patients, zygomatic implants present the most extreme version of the access problem: not only is the procedure expensive (CAD $70,000–$100,000 in private practice), but very few Canadian oral surgeons perform zygomatic implants at all. A patient in Halifax or Winnipeg told they need zygomatic implants may find no surgeon within 500 km with documented zygomatic case volume, meaning the treatment is effectively unavailable regardless of cost.
Zygomatic implant placement is performed by fewer than 50 surgeons in Canada, concentrated in major metropolitan centres, with extended wait times for consultation and limited surgical availability outside Toronto, Vancouver, and Montreal.
At Stunning Dentistry, the Dental Angel handover for zygomatic cases includes a GP letter explaining the sinus traversal, what nasal symptoms are expected, what warrants ENT referral, and the emergency contact number. Your Canadian doctor is not managing a procedure they have never heard of, they have a document that explains it.
Curious about costs and timelines?
CAD Cost Table
| Item | Stunning Dentistry (CAD) | Canadian Private (oral surgeon + prosthodontist) | Difference |
|---|---|---|---|
| Zygomatic implants (2) + standard (2) + provisional | $14,000–$20,000 | $45,000–$70,000 | ~$31,000–$50,000 |
| Quad-zygomatic (4 implants) + provisional | $18,000–$25,000 | $60,000–$85,000 | ~$42,000–$60,000 |
| Definitive zirconia prosthesis | $5,000–$8,000 | $15,000–$20,000 | ~$10,000–$12,000 |
| CBCT + zygomatic planning software | Included | $800–$2,000 | Included |
| ENT pre-surgical consultation | Included if required | $300–$800 | Included |
| Sedation (IV or GA) | $800–$1,500 | $2,000–$5,000 | ~$1,200–$3,500 |
| Return flights (Toronto–India economy) | $1,200–$1,800 | N/A | N/A |
| Accommodation (12–16 nights) | $1,000–$1,800 | N/A | N/A |
| **Total (hybrid config, complete)** | **~$22,000–$32,000** | **~$70,000–$100,000** | **~$45,000–$70,000** |
Want a personalised treatment plan?
Decision Framework
| Question | If Yes | If No |
|---|---|---|
| Is a Canadian zygomatic-trained surgeon available within reasonable distance? | Get a Canadian consultation first | Evaluate Stunning Dentistry, access is limited in Canada |
| Is the Canadian fee within budget without financial compromise? | Consider Canadian clinic | Evaluate Stunning Dentistry |
| Has CBCT confirmed Cawood & Howell Class IV–VI maxillary atrophy? | Zygomatic implants are indicated | Evaluate All-on-4 or All-on-6 first |
| Has pre-surgical ENT clearance been obtained if sinus pathology exists? | Proceed with surgical planning | Complete ENT workup before scheduling |
| Can you manage two trips (12–16 days + 5–7 days)? | Proceed | Discuss consolidated protocol |
Questions about this procedure?
Pre-Travel Checklist
| Item | Status |
|---|---|
| CBCT scan from Canadian clinic (if available) sent to Stunning Dentistry in advance | ☐ |
| ENT assessment results sent if sinus pathology history exists | ☐ |
| Full medical history form completed (systemic conditions, medications, prior dental surgery) | ☐ |
| Previous implant failure history disclosed with documentation | ☐ |
| Prior grafting attempts documented and sent | ☐ |
| Canadian GP briefed that zygomatic implant surgery is planned | ☐ |
| Canadian dentist briefed and willing to receive handover documentation | ☐ |
| Return flights booked: minimum 14 days for surgical trip, 5–7 days for definitive | ☐ |
| Accommodation arranged (Dental Angel can coordinate) | ☐ |
| Travel insurance covering surgical dental complications confirmed | ☐ |
| Saline nasal rinse (Neil Med equivalent) available for post-surgical use in India | ☐ |
| Emergency contact number for Stunning Dentistry saved | ☐ |
Ready to discuss your options?
Curious about costs and timelines?
Clinical References
1. Aparicio C, Manresa C, Francisco K, et al. Zygomatic implants: indications, techniques and outcomes, and the zygomatic success code. *Periodontol 2000.* 2014;66(1):41–58.
"name": "Stunning Dentistry"
Want a personalised treatment plan?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
I have been told I need bone grafting for regular implants. Does that mean I need zygomatic implants?
Not necessarily. CBCT evaluation determines whether your bone supports standard implants (with or without grafting) or whether zygomatic implants are the more appropriate protocol. Some patients told they need grafting for conventional implants are All-on-4 candidates. A subset with severe posterior atrophy require zygomatic implants. The imaging determines which path applies to you.
Can zygomatic implants be done for the lower jaw?
No. Zygomatic implants are exclusively a maxillary (upper jaw) procedure. There is no equivalent cheekbone anatomy in the mandible. Lower jaw atrophy is managed with standard All-on-4 or All-on-6 protocols, which work even in significantly resorbed mandibular bone.
How many trips to India does this require?
Two. The first trip (12–16 days) covers CBCT, ENT clearance if required, surgery, provisional fitting, and initial sinus recovery review. The second trip (5–7 days) at 5–7 months covers definitive prosthesis delivery.
What if I develop sinusitis after I return to Canada?
You receive a GP letter explaining your zygomatic implant case and the symptoms that warrant ENT referral. Mild sinus symptoms (nasal pressure, minor congestion) in the first 6 months are expected. Frank sinusitis (purulent discharge, facial pain, fever) warrants antibiotic treatment and ENT review, your Stunning Dentistry emergency contact is available 24/7 for guidance.
How is zygomatic implant surgery different from regular implant surgery?
The surgical corridor is different, the implant path is longer, the sinus is traversed, and anchorage is in the cheekbone rather than the alveolar ridge. This requires dedicated surgical instruments, specific anaesthetic planning (usually IV sedation or GA), and a longer operative time (typically 3–5 hours for a full arch). The recovery is also more substantial, greater facial swelling and a sinus adaptation period. ---
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










