Smile Design, Digital Smile Design + Veneer-Based Aesthetic Rehabilitation
- Smile Design exists because aesthetic dentistry spent decades trying to fix smiles one tooth at a time, and discovered that a beautiful smile is not a sum of beautiful teeth.
It is an architecture.
Overview
Smile Design exists because aesthetic dentistry spent decades trying to fix smiles one tooth at a time, and discovered that a beautiful smile is not a sum of beautiful teeth. It is an architecture. The relationship between upper lip and incisal edge. The curve of the incisal plane against the lower lip. The gingival zeniths that sit higher on the canines than the centrals. The midline. The buccal corridor. The phonetic position of the "F" and "V" sounds. Change one of these in isolation and the smile still looks wrong, even if every tooth has been restored with the most expensive material available.
This is not a shortcut. It is an engineered protocol backed by more than three decades of clinical evidence, Beier's 20-year veneer survival data, Galip Gurel's Aesthetic Pre-Recontouring (APR) technique, Pascal Magne's bonded porcelain longevity studies, and the Coachman Digital Smile Design protocol that made the discipline teachable across thousands of clinics worldwide.
For patients reading from Canada
The Smile Design workflow you receive at Stunning Dentistry is the same protocol offered in leading aesthetic practices in Toronto, Vancouver, Montreal, and Calgary. Developed from the academic work of Frush & Fisher, Lombardi, Chu, Coachman, Gurel, and Magne. Executed with Emax lithium disilicate, feldspathic porcelain, or monolithic zirconia. Designed in DSD App, Exocad, or 3Shape. Bonded under rubber-dam isolation with Variolink or RelyX cements. What changes when you travel is not the clinical protocol, it is the specialist bench you access, the in-house ceramist capacity, and the total cost. We walk through exactly how that comparison lines up further down this page.
At Stunning Dentistry
Every Smile Design case is opened in the DSD App with a two-minute video of you speaking, smiling, and laughing, before any tooth is touched. Your proposed incisal edge position is overlaid against your upper lip in motion, not just against a static photograph. The prosthodontist, the cosmetic lead, and the master ceramist all sign off on the digital design before the mock-up is printed. That three-person review is the single biggest reason our aesthetic outcomes hold up at the five-year and ten-year follow-ups instead of drifting.
What Is Smile Design?
Smile Design is a structured, evidence-based protocol for planning and executing aesthetic rehabilitation of the teeth visible in speech and smile. It is not a single procedure, it is a design framework within which several procedures may be used, always orchestrated to the same engineered outcome.
The Architectural Design
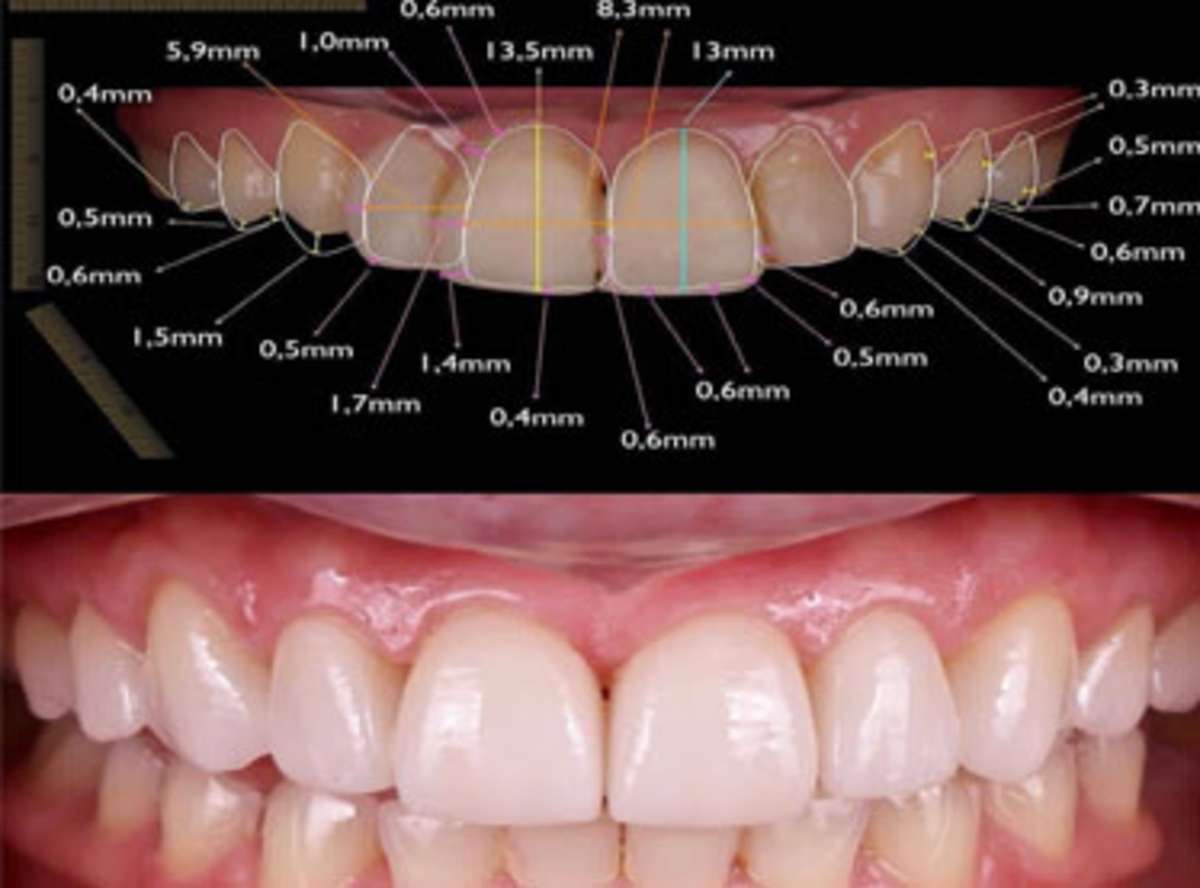
- Facial midline to dental midline alignment, the dental midline should sit within 2 mm of the facial midline and be vertical within 2 degrees (Kokich et al., aesthetic deviation studies)
- Incisal edge position, determined against the relaxed upper lip and the phonetic "F/V" position, which reveals the wet-dry border of the lower lip and anchors where the incisal edge must finish
- Width-to-length ratio, central incisors at approximately 75–80% width-to-length (Chu's proportions)
- Golden proportion and RED proportion, the recurring esthetic dental proportion (Ward) where each tooth appears 70% the width of its mesial neighbour from the frontal view, giving the eye a natural recession into the buccal corridor
- Gingival zenith architecture, canine zeniths higher than central zeniths, laterals approximately 1 mm lower, with parallelism to the incisal plane
- Smile arc, Frush & Fisher's curved smile arc where the incisal edges of the upper anteriors follow the curvature of the lower lip on smiling
- Buccal corridor, the dark space lateral to the premolars that, when too wide, makes the smile appear narrow; Smile Design widens premolars proportionally to close this
- Tooth proportion within the visible smile, centrals dominant, laterals subordinate, canines with character, premolars receding
The design is tested as a physical mock-up made from a putty matrix of the diagnostic wax-up. You wear it for 48 to 72 hours. You speak, eat, smile, photograph, and share it with your partner. You approve it, or you request changes. Only after approval do we prepare any teeth.
What Smile Design Is Not
- It is not a whitening procedure
- It is not a single-tooth repair
- It is not same-day cosmetic composite bonding without planning
- It is not an Instagram filter applied with porcelain
- It is a fully diagnostic, digitally engineered, mock-up-validated aesthetic reconstruction of the smile as a functional, facial-integrated system
At Stunning Dentistry
We decline Smile Design cases where the patient arrives with a reference photograph of another person's teeth and asks for that exact smile. We will borrow shape elements, character elements, and proportional guidance from a reference, but the smile we design will be yours, matched to your face shape, your lip line, your phonetic position, your age, and your personality. A twenty-six-year-old's centrals are not a fifty-two-year-old's centrals, and a Mediterranean face is not a Northern European face. We design from your starting point, not from a screenshot.
Why Choose Smile Design, The Clinical Case
When a patient presents with an aesthetically compromised smile, discoloured teeth, worn edges, uneven gingival heights, old composite repairs turning dark, peg-shaped laterals, a gummy smile, or a collapsed bite from years of wear, the realistic options are: do nothing, whiten only, composite bonding on individual teeth, isolated veneers on the visible teeth only, orthodontic pre-treatment followed by veneers, or a fully planned Smile Design that treats the smile as a system. Each has clinical indications. Here is why, for the majority of cosmetically-motivated patients with multiple concerns, Smile Design is the most defensible choice.
1. It Fixes the Smile, Not the Teeth
2. The Mock-Up Approval Gate Eliminates Surprise
3. Minimum Prep and No-Prep Options Preserve Tooth Structure
4. The Digital Workflow Makes Outcomes Reproducible
5. Three Decades of Published Outcome Data
6. Occlusal Engineering Protects the Investment
7. Specialist-Executed, Reproducible Across the Team
Smile Design is not a one-person discipline. It requires a prosthodontist for treatment planning, a cosmetic lead for shade and shape execution, and a master ceramist for final layering. At Stunning Dentistry, the three meet in the same building for every aesthetic case. The chair-side adjustments, the shade matches, and the shape refinements happen in real time instead of bouncing between a clinic and an outsourced laboratory.
At Stunning Dentistry
We decline aesthetic cases where the clinically correct answer is orthodontics rather than veneers. If your concern is crowding that Invisalign can resolve in nine months, we will send you home with an aligner referral before we prepare your enamel. Preserving your natural teeth is almost always the better long-term outcome. We write that into every consultation note, and our decline rate on single-concern crowding cases sits above fifteen per cent. The protocol serves the patient, not the other way around.
Why Digital Smile Design Changes the Outcome
The single most important innovation in modern aesthetic dentistry is the move from analogue, intuitive planning to digital, facial-integrated design.
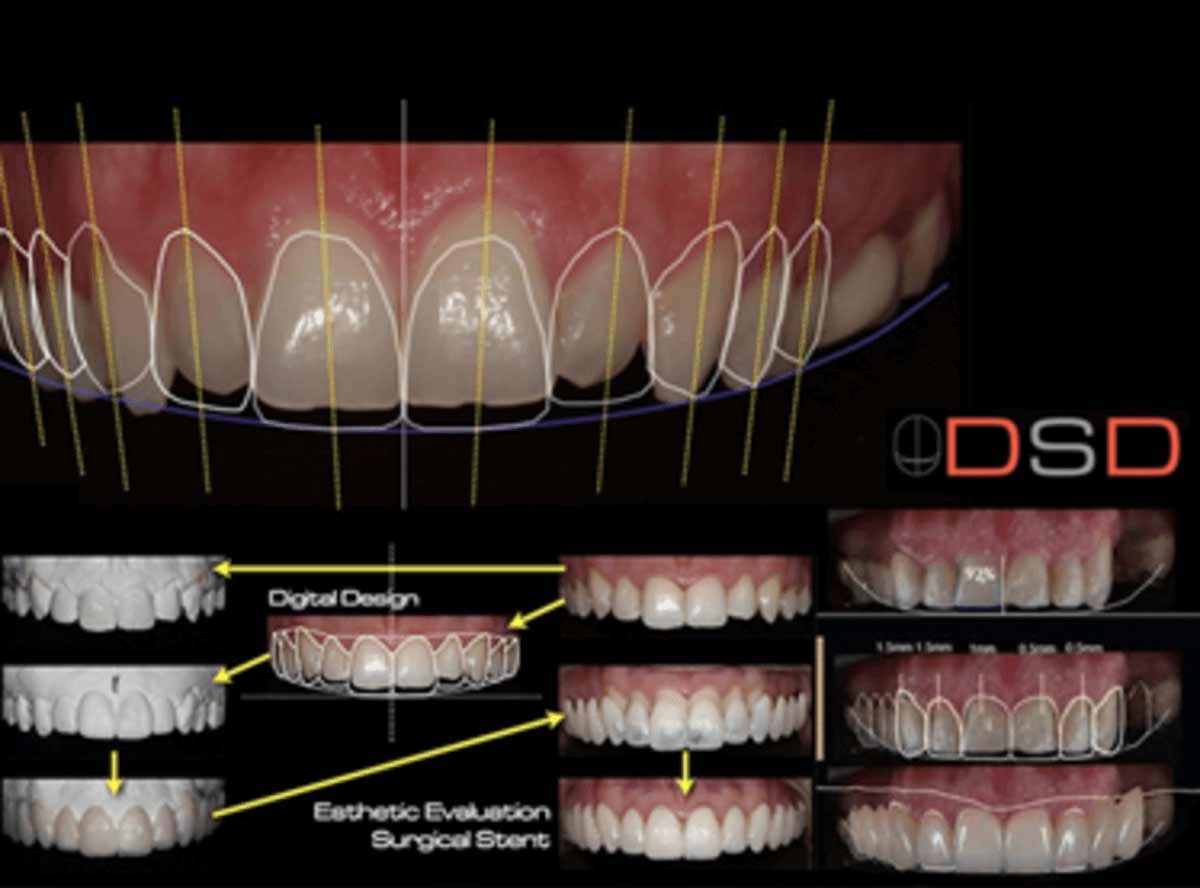
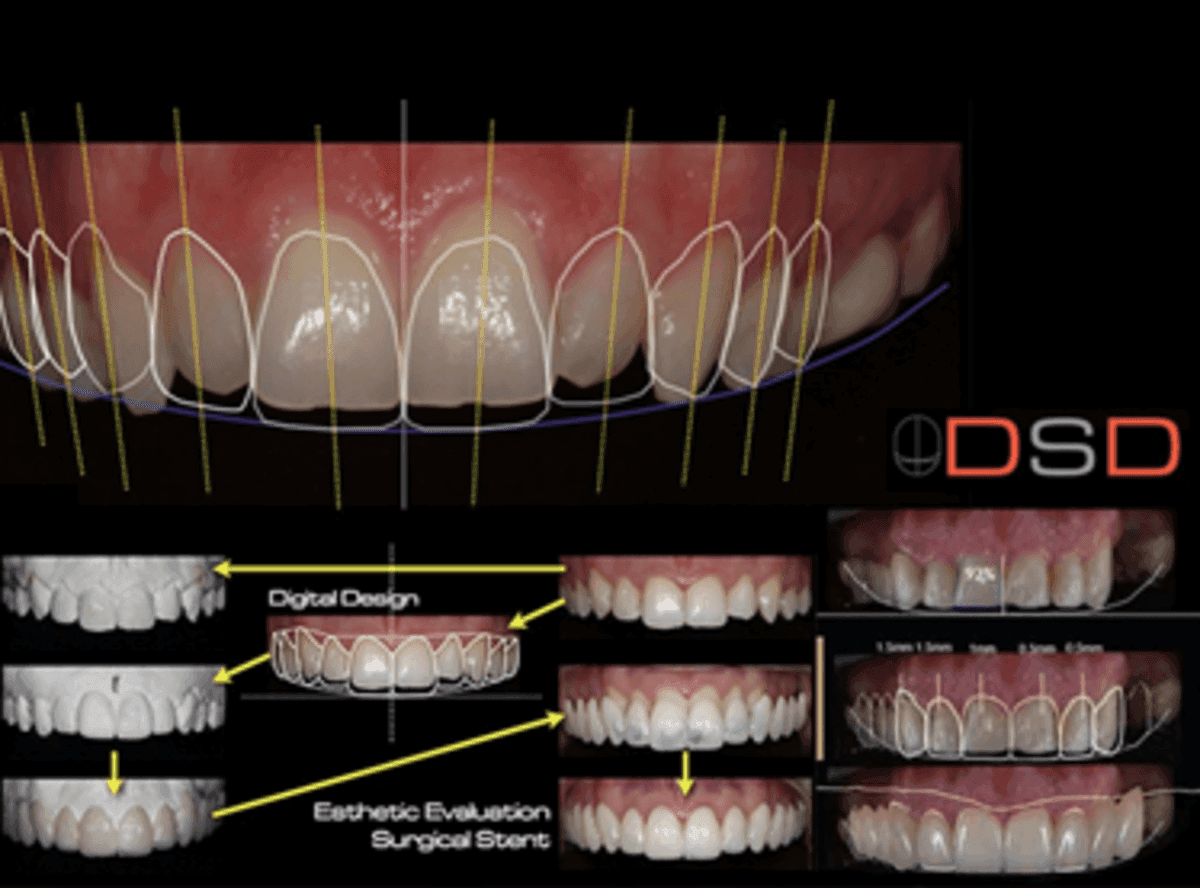
- Facial-referenced midline and incisal edge planning, the design is drawn against your face, not your cast
- Dynamic smile integration, the incisal edge is positioned against your lip in motion, not in a static pose, eliminating the "static-smile trap" that produces teeth too long on camera
- Patient communication that is visual, not verbal, the patient sees the proposed smile on their own photograph before any tooth is touched
- Reproducible transfer from digital plan to physical mouth, the 3D-printed wax-up, the silicone mock-up matrix, and the final ceramic all reference the same digital source file
- Objective shade mapping, cross-polarised photography and spectrophotometric measurement eliminate the subjective shade-guide-under-operatory-light problem that produced a generation of mismatched anterior restorations
At Stunning Dentistry, the DSD App runs on iPads in every cosmetic operatory, and every case is also rendered in Exocad Smile Creator by the in-house digital technician. The two environments cross-check each other. Where they disagree, the case is paused until the master ceramist resolves the disagreement manually.
At Stunning Dentistry
Our Smile Design workflow begins with an 84-megapixel full-face reference photograph, a cross-polarised 1:1 anterior photograph, and a slow-motion smile video at 240 frames per second captured on a calibrated iPhone with a dental-specific colour reference in frame. Those three records go into the DSD App the same afternoon. If any of the three cannot be captured cleanly, we pause and retake. The design is only as good as the input data, and we do not compromise the input.
Long-Term Survival Data
Smile Design is one of the most extensively studied domains in aesthetic dentistry, porcelain veneers specifically have nearly forty years of published follow-up data.
Porcelain Veneers (Feldspathic and Pressed Ceramic)
- Cumulative survival at 10 years: 95.2%
- Cumulative survival at 20 years: 82.9%
- Most common failure mode: ceramic fracture (67% of all failures), followed by loss of bond and secondary caries
- Major risk factor for failure: bruxism and parafunction (relative risk 7.7 times higher than non-bruxers)
- Enamel vs dentine bonding: veneers bonded entirely to enamel showed significantly better survival than veneers bonded to dentine-exposed preparations
Lithium Disilicate (Emax) and Pressed Ceramic Restorations
- 5-year survival: 94–98% across multiple studies
- 10-year survival: 90–95% for veneers, 93–97% for crowns
- Primary failure mode for veneers: fracture
- Primary failure mode for crowns: loss of retention or secondary caries
- Monolithic lithium disilicate showed superior fracture resistance compared to layered porcelain-fused-to-zirconia in posterior aesthetic crowns
Composite Veneers
- 5-year survival: 85–93% for indirect composite veneers
- 10-year survival: 65–75% for direct composite veneers
- Primary failure mode: surface staining, chipping at incisal edge, and loss of polish
- Repair advantage: composite veneers can be repaired intraorally; porcelain veneers generally require replacement when fractured
Minimally Invasive (No-Prep and Minimum-Prep) Veneers
Gurel G et al. (2013), Aesthetic Pre-Recontouring technique, 5-year follow-up:
- Survival at 5 years: 96% with APR protocol
- Enamel preservation: 60–70% of original enamel thickness retained
- Patient-reported aesthetic outcome: 97% satisfaction at 5 years
At Stunning Dentistry
Every aesthetic patient enters our internal outcomes registry on the day of delivery. Shade at delivery, margin integrity at 6 months, surface texture at 12 months, occlusal wear at 24 months, patient-reported satisfaction at 12 and 36 months. We benchmark our survival rates against the Beier 20-year dataset and the Gurel APR dataset, and we publish the internal audit annually to our clinical board. Where our numbers drift below the published benchmark, the case is reviewed by the master ceramist and the prosthodontist to identify the protocol adjustment required.
Clinical Equipment & Technology
A predictable case is only as good as the planning and fabrication stack behind it. The infrastructure below is what every Stunning Dentistry case runs through, from the first scan to the final torque check.
What Patients Are Buying When We Quote a Case
For the full equipment showcase including sterilisation, smile-design tooling, and the case-documentation registry, see Our Clinical Equipment & Technology.
At Stunning Dentistry
Every fixture placement on a Canadian case carries an insertion-torque value (typically 35–65 Ncm) and an ISQ reading (target ≥ 68 at second stage) recorded on the patient file. 1 mm. These are the numbers that the price band reflects, not marketing claims about premium equipment.
| System | Stunning Dentistry stack | What it controls in your case |
|---|---|---|
| Cone-Beam CT | Carestream / Planmeca CBCT | Bone density (HU), ridge width, sinus floor distance, IAN canal proximity |
| Intraoral scanner | 3Shape TRIOS 5 | Margin-line capture, occlusal record, soft-tissue contour |
| Planning software | coDiagnostiX, NobelGuide | Virtual implant placement, surgical-guide design, prosthetic-driven backward planning |
| Digital articulator | Modjaw / JMA Optic | Mounted bite registration, jaw-relation validation before definitive |
| Surgical motors + guides | Nobel Biocare / Straumann surgical kits | Insertion-torque measurement, ISQ resonance frequency analysis |
| 5-axis milling | Roland DWX / VHF S2 | Monolithic zirconia framework precision (≤ 25 µm marginal fit) |
| 3D printing | Formlabs Form 3B+ | Surgical guides, provisionals, try-in models |
| Implant systems | Nobel Biocare + Straumann (primary) | Fixture range covering bone densities D1–D4, immediate-load thresholds |
Symptoms and Signs That Indicate You May Need Smile Design
Most patients do not arrive at a Smile Design consultation after a single event. They arrive after years of accumulated aesthetic compromise, the tetracycline staining from childhood antibiotics, the composite bondings done in the thirties that have turned grey, the wear from nocturnal bruxism, the gingival recession that exposes dark root surfaces, the old crowns that no longer match adjacent teeth. The smile fails gradually, and then one day a clinical threshold is crossed.
Colour and Shade Signs
- Your teeth have darkened despite regular whitening, and the change has not responded to bleaching in the past 12 months
- Tetracycline staining that whitening cannot reach, grey, brown, or banded discolouration through the dentine
- Fluorosis, chalky white or brown patches across multiple teeth from childhood water exposure
- Old composite fillings in the anterior teeth that have turned darker, yellower, or more grey than the surrounding natural tooth
- A single dark tooth from a previous root canal that no longer matches the rest of the smile
- Internal staining visible through translucent enamel from dentine discolouration
Shape and Position Signs
- Teeth that look too short for your face, centrals under 9 mm in length or showing less than 3 mm of incisal display in a relaxed smile
- Teeth that appear too long, worn lower incisors with chipped edges, or upper anteriors that have supra-erupted into a collapsed bite
- Peg-shaped lateral incisors that never reached full size
- Microdontia, teeth that are proportionally smaller than the arch they sit in, producing visible gaps
- Mild crowding you do not want to treat orthodontically, where the anterior teeth rotate or overlap by 1–2 mm
- Diastemas, small midline gaps or post-orthodontic space that has reopened
Wear and Structural Signs
- Flat, sharp, or chipped incisal edges from bruxism, clenching, or acid erosion
- Shortened upper anteriors from decades of parafunction
- Exposed dentine visible on the biting edges of incisors
- Notching at the gumline of premolars and canines (abfraction)
- Old crowns with visible dark margins where the gum has receded
- Ceramic chipping on existing veneers, crowns, or bridges
Gingival Signs
- Uneven gumline, one central sits higher or lower than its mirror tooth
- Excessive gingival display on smiling ("gummy smile") with more than 3 mm of gum showing
- Short clinical crowns with adequate root length, candidates for crown lengthening
- Black triangles between teeth where the papillae have been lost to gum recession or orthodontic contraction
- Discoloured or blue-tinted gingiva over old PFM (porcelain-fused-to-metal) crowns
Psychological and Social Signs
- You cover your mouth when you laugh
- You avoid being photographed, or turn your head so only a profile is captured
- You have declined speaking roles at work, weddings, or social events because of how your smile looks on camera
- Your confidence has measurably shifted over the years as the smile has deteriorated
- You have started wearing darker lipstick or a specific shade of lipstick to draw attention away from your teeth
If three or more of the above apply to you, a Smile Design consultation is appropriate. The earlier the evaluation, the more options remain, minimum-prep and no-prep protocols are only available when the enamel is still intact and the bite has not yet collapsed.
At Stunning Dentistry
The first Smile Design consultation is diagnostic, not transactional. We take a full facial photograph set, cross-polarised intraoral series, slow-motion smile video, intraoral scan, and a bite analysis on the same day. " Many Canadian patients leave that first consult with a plan that includes Invisalign before veneers, because preserving your enamel is almost always the right first call.
Who Is a Candidate?
Ideal Candidates
- Patients with discoloured anterior teeth (tetracycline, fluorosis, endodontically treated, age-related dentine darkening) where bleaching has plateaued
- Patients with worn dentition from bruxism, parafunction, GERD, or dietary acid erosion who have lost vertical dimension and smile architecture
- Patients with mild to moderate crowding who decline orthodontic treatment and accept the trade-off of veneer-based correction
- Patients with old composites that have discoloured, chipped, or failed at the margins
- Patients with black triangles, uneven gingival heights, excessive gingival display, peg laterals, or microdontia
- Patients in stable periodontal condition with no active decay
- Patients who understand this is a lifetime commitment with predictable replacement cycles
Relative Contraindications
- Severe uncontrolled bruxism, must be managed with occlusal splints pre-treatment and night guards post-treatment; in extreme cases, ceramic is not the right material and we will recommend a different plan
- Active periodontal disease, must be resolved before aesthetic work is planned, as subgingival margins on inflamed tissue produce chronic failure
- Inadequate enamel, patients whose enamel has been over-reduced by previous dentistry, or whose teeth are already largely dentine-based, are at higher debonding risk; a full-coverage crown may be the better restoration
- Pregnancy, elective aesthetic work is typically deferred to post-partum
- Unrealistic reference images, patients who arrive with a photograph of a celebrity smile they expect to match exactly on a different face shape are not good candidates for Smile Design in its honest form
- Active caries or uncontrolled decay risk, the underlying disease must be addressed before the aesthetic restoration
- Patients under 18 with developing dentition and incomplete facial growth, smile architecture changes through early twenties
Medical Evaluation
Suitability is determined by dental health, parafunctional profile, and aesthetic appetite more than chronological age. The Beier 20-year dataset included patients across a wide age range with successful long-term outcomes. Evaluation at Stunning Dentistry includes digital intraoral scanning, CBCT for any teeth with prior endodontic treatment, full periodontal charting, bruxism assessment with muscle palpation and occlusal wear mapping, and a detailed aesthetic expectations interview.
At Stunning Dentistry
Candidacy for Smile Design is decided by a three-person clinical review: a prosthodontist, a cosmetic lead, and the master ceramist read every case together before treatment is confirmed. If any of the three flags a concern, enamel too thin for the planned preparation, bruxism not under control, expectations misaligned with what ceramic can honestly deliver, the case is paused and resolved first. We have turned down Smile Design cases we could have accepted because the long-term outcome was unlikely. That is the filter we run.
Consequences of Delaying Aesthetic Treatment
The cost of waiting on a compromised smile is not measured in dollars. It is measured in enamel, in tooth wear, in the surgical complexity of the case when you finally decide to act, and in the years you spend hiding a smile you would rather show.
What Happens to the Enamel
- Bruxism wear rates: 0.03 to 0.1 mm per year in mild bruxers, up to 0.3 mm per year in severe nocturnal bruxers
- Dietary acid erosion: citrus, wine, carbonated drinks, and sports drinks can strip 0.1 to 0.2 mm of enamel per year with daily exposure
- GERD and silent reflux: palatal surface erosion on upper anteriors is often the first visible sign of undiagnosed acid reflux
What Happens to the Bite
- Lower incisors over-erupt into the space left by worn upper incisors
- The bite deepens, trapping food on lingual surfaces
- Temporomandibular joints experience abnormal loading patterns
- What started as a single aesthetic concern becomes a full-mouth rehabilitation
What Happens to the Face
- The chin appears to move closer to the nose
- The nasolabial folds deepen
- The corners of the mouth turn down at rest
- The patient appears 5 to 10 years older than chronological age
What Happens to the Treatment Cost
- A ten-year delay on a bleaching-plus-minimum-prep-veneers case may convert it into a full-coverage-crowns-with-crown-lengthening case, typically doubling or tripling the fee
- Untreated bruxism compounds ceramic failure risk once restorations are finally placed, requiring a pre-treatment phase of occlusal splint therapy
- Dentine exposure from continued wear moves the bonding surface away from enamel, reducing long-term reliability
- Pulp exposure risk increases with continued wear, adding endodontic treatment to the plan
The earlier the case is treated, the simpler the protocol and the lower the total investment over a lifetime.
At Stunning Dentistry
We are honest about delay. Most aesthetic concerns do not require urgent treatment. But some do, and the difference between "monitor for a year" and "intervene now" is clinical, not promotional. If your enamel is visibly thinning, if your bite is collapsing, or if your bruxism is actively destroying the edges of your teeth, the time to act is when the enamel is still there to bond to. We tell patients what their honest window is. We do not accelerate decisions that do not need accelerating.
Mock-Up to Motion: Testing Your New Smile Before It's Permanent
The most important innovation in modern Smile Design is the mock-up approval gate, the protocol step that separates surgical cosmetic dentistry from Instagram cosmetic dentistry.
- The diagnostic wax-up is scanned or manually shaped on a plaster model
- A silicone putty matrix is taken of the wax-up
- Bis-acrylic composite resin is injected into the matrix and seated over the patient's unprepared teeth
- The resin sets in minutes, producing a physical, millimetre-accurate copy of the proposed smile directly on the patient's teeth
- The patient wears the mock-up for 48 to 72 hours
- The patient speaks, eats soft foods, photographs themselves, shows friends and family, and confirms phonetic performance (F, V, S sounds especially)
- The patient returns for an approval appointment where any change is captured in writing before the mock-up is removed
There are situations where a mock-up is not sufficient on its own, cases involving major vertical dimension change, significant crown lengthening, or orthodontic pre-treatment. In those cases, the mock-up is extended into a longer-wear provisional worn for 2 to 8 weeks while the jaw adapts, the gingiva heals, and the patient lives with the new smile in full function before final restorations are fabricated.
At Stunning Dentistry
The mock-up you wear for 48 hours before we prepare anything is not a sales gimmick. It is a contractual approval gate. Every final restoration must match the mock-up we both signed off on, in writing, on Day 2. If the mock-up is wrong, if the length feels too long, the shape feels too square, the shade feels too white, we adjust the wax-up and re-mock-up before any irreversible step. We have re-done mock-ups three times on a single case. We would rather remake the wax-up than remake the ceramic.
Same-Day Aesthetics, Digital Preview to Delivery
One of the defining features of the modern Smile Design protocol is the ability to preview, prepare, and provisionalise the smile within a compressed same-day or same-week window, without sacrificing the quality of the final restoration.
What Same-Day Aesthetics Requires
- A fully digital front-end: intraoral scanner (3Shape TRIOS or iTero) capturing the prepared teeth at sub-20-micron resolution
- DSD App or Exocad Smile Creator running the design against the facial photograph
- In-house 3D printer (Formlabs Form 3B or equivalent) producing the bis-acrylic mock-up and printed try-in
- In-house CAD/CAM mill (Roland DG or Sirona inLab) for provisional PMMA restorations or single-visit lithium disilicate crowns
- A master ceramist on site for chair-side shade characterisation when staining, glazing, or micro-layering is required
The Provisional Phase
- Verifies the new incisal edge position against lip motion
- Allows phonetic adaptation, F, V, S sound positions
- Tests occlusal function under real-world chewing
- Confirms gingival response to new emergence profiles
- Provides time for the patient to take photographs in different lighting and confirm shade in daylight, in indoor office light, and on camera
After the provisional phase (typically 3 to 10 days in an international patient workflow, longer in a domestic phased case), the final ceramic restorations replace the provisionals under rubber-dam isolation with resin-based cementation.
At Stunning Dentistry
"same day" is not a promise we make. It is a capability we have. Whether a case is completed in a single visit, a week-long compressed visit, or a staged two-visit protocol depends on the clinical complexity, not on what the patient saw on social media. Lithium disilicate requires a specific sintering and glazing cycle. Master-ceramist hand-layered feldspathic porcelain requires bench time that cannot be compressed. We will deliver the smile in the timeline the material and the case honestly require, not in the timeline that sounds most impressive.
Benefits of Smile Design, What You Get That Single-Tooth Cosmetics Do Not Deliver
The clinical literature catalogues outcomes. Patients live with outcomes. Here is the lived difference, the set of things patients report gaining from a properly executed Smile Design that isolated cosmetic dentistry cannot provide.
An Architecturally Coherent Smile, Not a Set of Matching Teeth
Full Bite Force and Functional Stability
Colour Stability Against Coffee, Wine, and Tea
Restored Facial Dimension Where Wear Has Collapsed It
Clear, Confident Speech
Easier Long-Term Hygiene
Documented 10–20 Year Service Life
Psychological Outcome
The published quality-of-life data from the OHIP-14 (Oral Health Impact Profile) and the Psychosocial Impact of Dental Aesthetics Questionnaire show statistically significant gains after Smile Design: increased self-esteem, reduced social avoidance, increased self-reported attractiveness, and improved mental wellbeing scores at 12 and 24 months post-treatment. The smile is tied to identity more than any other facial feature. Restoring it restores more than teeth.
At Stunning Dentistry
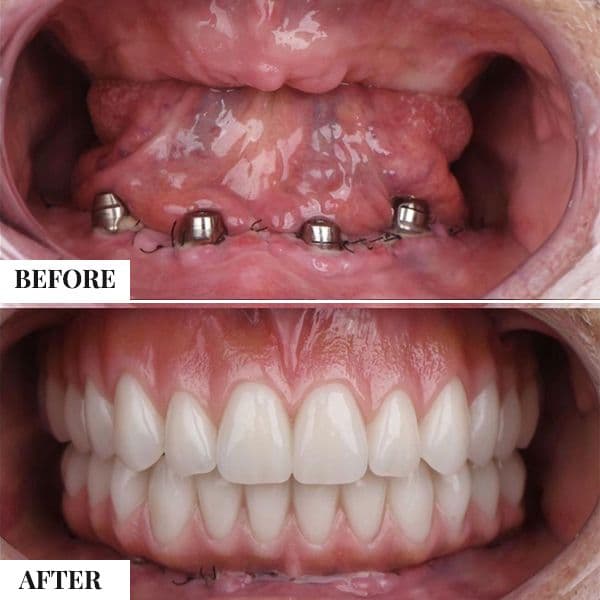
Every aesthetic patient is photographed at delivery and at every annual review with a standardised cross-polarised camera setup, calibrated colour chart in frame, and identical lighting conditions. The photographic record is the objective measure against which any shade drift, margin staining, or incisal wear is tracked. Before-and-after is not marketing at our clinic. It is clinical documentation, filed in your chart, available to you on request at any review.
Recovery Timeline, Day 1 to Year 1
A structured day-by-day and week-by-week view of what happens inside your mouth and inside your life after Smile Design. The aesthetic workflow is very different from the surgical recovery of an implant case, there is no deep tissue healing, but there is a meaningful adaptation phase as the jaw, lips, and speech adapt to the new aesthetic architecture.
Day 0, Preparation and Temporaries Placed
- Local anaesthesia for the preparation appointment (minimum-prep cases often require very light anaesthesia or none; conventional-prep cases require standard local block or infiltration)
- Teeth are prepared to the depth dictated by the wax-up, typically 0.3–0.5 mm for minimum-prep veneers, 0.7–1.0 mm for conventional veneers, 1.2–1.5 mm for full-coverage crowns
- Intraoral scan captures the prepared teeth
- Provisional restorations fabricated in PMMA in-house and cemented with spot-etch temporary bonding
- Patient leaves with a full aesthetic provisional set, not a "stub teeth" appearance
Days 1–3, Adaptation Window
- Mild sensitivity to cold and sweet on the prepared teeth, managed with desensitising paste and a short course of ibuprofen if needed
- Soft tissue tenderness at the gingival margins from retraction cord placement, resolves within 48 hours
- Phonetic adaptation begins, the tongue finds the new incisal edge position within 24 hours
- Diet remains soft, avoid hard, sticky, or coloured foods (red sauces, curry, coffee) that can stain the provisional PMMA
- First photograph check, take a selfie to confirm the provisional shape in your own lighting
Days 4–7, Settled Provisional Phase
- Sensitivity typically resolves by day 4–5
- Phonetics normalise, F, V, S sounds all return to natural range
- Patient adjusts to the new lip support; initial perception of "teeth too long" usually resolves within a week
- Soft-chewable diet expands, pasta, well-cooked vegetables, soft protein
- International patients typically have their try-in appointment during this window
Days 7–10, Try-In and Final Cementation
- Try-in appointment: final ceramic restorations are placed without cement to confirm shape, shade, fit, and bite
- Patient approval is explicitly captured before cementation, the final chance to request any shape or shade adjustment
- Final cementation under rubber-dam isolation using adhesive resin cement (Variolink, RelyX, or Panavia V5 depending on ceramic type)
- Light-cure protocol verified for each tooth
- Occlusal adjustment with articulating paper and T-Scan digital occlusal analysis
- Post-cementation photograph taken for the file
Week 2, Settled Function
- Full aesthetic function restored
- Patient can eat full diet including hard fruits, nuts, and raw vegetables, with the caveat that incising hard objects (ice, bones, pen caps) is never recommended for any ceramic restoration
- Coffee, tea, red wine, and curry can be consumed normally, ceramic does not absorb stain
- Bite continues to settle; minor adjustments may be needed at the 2-week review
- Night guard is fabricated and delivered (in a same-visit workflow this happens at the Day 7–10 window; in staged cases it may be sent home with a digital impression for lab fabrication)
Weeks 3–8, Soft Tissue Finalisation
- Gingival tissues around the veneer margins fully settle, any mild inflammation from preparation resolves
- Papillae fill to their final height, particularly important where gingival contouring was performed
- Patient reports feeling "the veneers are mine" rather than "I am wearing veneers", a subjective but consistent milestone around the 4–6 week mark
- First professional hygiene appointment (if timing allows) reinforces cleaning technique
Month 3, First Review
- Clinical examination of margins, gingival response, and occlusal wear on the night guard
- Cross-polarised photograph to compare against delivery-day baseline
- Patient-reported outcome measure captured
- Any minor occlusal refinement performed
Month 6, Mid-Year Review
- Second set of photographs
- Hygiene reinforcement
- Night guard inspection
- Discussion of any patient-reported concerns
Month 12, First Annual Review
- Comprehensive clinical examination
- Cross-polarised photograph series (same calibration as delivery)
- Bite analysis and any required occlusal adjustment
- Night guard fit verified, if the patient has gained or lost weight, or if muscle patterns have changed, a new guard may be indicated
- Baseline established for lifetime monitoring
At Stunning Dentistry
The three-month, six-month, and twelve-month reviews are booked into the same clinical calendar as our surgical cases. Canadian patients complete these reviews by structured Zoom with photograph upload; those within India attend in person. The same prosthodontist who delivered your smile reviews every photograph. We do not hand you off to a dental nurse or a general practitioner for post-delivery monitoring. Continuity is the mechanism through which long-term aesthetic outcomes hold up.
Complications and How They Are Managed
No aesthetic protocol is free of complications. The Smile Design literature is transparent about this, and we publish our own numbers against it.
Debonding
- Incidence: 2–5% at 10 years for porcelain veneers bonded to enamel; higher (up to 8–12%) for veneers bonded to partial dentine
- Primary cause: inadequate bonding substrate (dentine exposure), contamination during cementation, or parafunctional overload
- Management: re-bond under rubber-dam isolation if the veneer is intact and the substrate is clean; replace if the ceramic is contaminated or the substrate is compromised
- Prevention at Stunning Dentistry: rubber-dam isolation for every cementation, total-etch enamel protocol where enamel is the primary substrate, master ceramist on site for immediate troubleshooting
Chipping and Fracture
- Incidence: the most common failure mode per Beier's 20-year data, 67% of all veneer failures
- Primary cause: bruxism, clenching, trauma (falls, sports), or bite overload
- Risk factor: unmanaged parafunction is the single largest predictor (relative risk 7.7 times higher in bruxers)
- Management: small marginal chips can often be polished or repaired with composite; larger fractures typically require veneer replacement
- Prevention at Stunning Dentistry: a night guard is fabricated and delivered for every Smile Design patient. Non-negotiable. Full-coverage hard acrylic, or a dual-laminate construction for heavy bruxers.
Post-Preparation Sensitivity
- Incidence: 10–20% of minimum-prep veneer patients experience transient sensitivity in the first 2–4 weeks
- Primary cause: dentinal tubule exposure at preparation margins
- Management: desensitising paste (SensiKin, Tooth Mousse), fluoride varnish, short course of NSAIDs if needed
- Typical resolution: 2–6 weeks; persistent sensitivity beyond 12 weeks warrants review
Pulpal Injury
- Incidence: <1% with minimum-prep protocols; 2–4% with conventional full-coverage crown preparations
- Primary cause: aggressive tooth reduction, particularly on younger teeth with larger pulp chambers
- Management: vital pulp therapy, or root canal treatment if pulpitis becomes irreversible
- Prevention: CBCT imaging for any tooth over age 40 or with prior deep restorations; preparation depth guides; no free-hand over-preparation
Shade Mismatch
- Incidence: reported patient dissatisfaction with final shade in 3–7% of cases in older workflows, reduced substantially in DSD-driven workflows with cross-polarised photography and spectrophotometric mapping
- Primary cause: subjective shade selection under operatory lighting that differs from daylight
- Management: veneer replacement is the only definitive fix; external staining and glazing can achieve minor corrections
- Prevention at Stunning Dentistry: every shade is captured with cross-polarised photography, a spectrophotometric reading from a handheld device, and a bench-top shade match under corrected daylight lighting
Gingival Response to Margins
- Incidence: 5–10% of cases report transient gingival inflammation at veneer margins in the first 4–8 weeks
- Primary cause: overcontoured emergence profile, subgingival margin placement where supragingival would have sufficed, or rough marginal finish
- Management: marginal refinishing, improved home hygiene, chlorhexidine rinse short course
- Prevention: supragingival margins wherever aesthetically acceptable; margins placed precisely at the free gingival margin where subgingival is required
Black Margins on Older Crowns (Historical Issue)
- Incidence: seen in older porcelain-fused-to-metal (PFM) crowns where gingival recession exposes the metal substructure
- Relevance to Smile Design: patients presenting with old PFM crowns in the aesthetic zone are offered replacement with all-ceramic (lithium disilicate, zirconia, or feldspathic) as part of the Smile Design plan
- Prevention: we do not place PFM in the aesthetic zone, ceramic throughout the smile line
At Stunning Dentistry
We publish our complication profile to every Smile Design patient before treatment begins. 8% across 1,400 veneers placed between 2018 and 2023. 4%, concentrated in patients whose night guard compliance was documented below 80%. These are our numbers, not industry averages. If your question is "what happens when it fails," the response is already written in your warranty document on the day you receive the smile.
Smile Design vs Single-Issue Cosmetic Dentistry
Single-issue cosmetic dentistry is appropriate, and it is what we recommend, when the problem is genuinely a single tooth. A single fractured central incisor in a forty-five-year-old with otherwise healthy, well-proportioned teeth does not need a Smile Design. It needs one excellent veneer matched carefully to its neighbours. When more than three or four teeth are involved, or when the architecture itself is compromised, Smile Design becomes the more defensible protocol.
At Stunning Dentistry
We are just as willing to tell a patient "you need one veneer, not ten" as we are to plan a full Smile Design. Over-treatment is a cosmetic-dentistry failure mode as serious as under-treatment. A case that calls for a single-tooth match should be treated as a single-tooth match, and the clinician who knows that is the one to trust with your aesthetic work.
| Factor | Smile Design (Full Planning) | Single-Issue Cosmetic (Veneer-by-Veneer) |
|---|---|---|
| Planning approach | Face-referenced digital design of the entire smile | Tooth-by-tooth response to individual concerns |
| Mock-up approval | Mandatory physical mock-up worn for 48–72 hours | Usually none, or wax-up photograph only |
| Restoration count | 8–20 teeth treated as a coherent unit | Often 2–4 teeth treated in isolation |
| Midline and architecture | Planned against the face | Inherits whatever the existing teeth provide |
| Occlusal integration | Full bite analysis, articulator mount, night guard | Usually addressed only if a problem emerges |
| Predictability | High, outcome matches the approved mock-up | Variable, depends on interpretation at the chair |
| Long-term aesthetic coherence | Consistent across 10–20 years | Risk of mismatched shades as teeth age at different rates |
| Cost | Higher upfront; lower lifetime cost per aesthetic-year | Lower upfront; higher lifetime cost due to replacement mismatches |
| When it is the right call | Multi-concern cases, full-mouth aesthetic compromise, new-build smile | Single fractured or discoloured tooth adjacent to otherwise good dentition |
Smile Design vs Alternatives, The Full Ladder
Aesthetic dentistry is not a one-size decision. The right protocol depends on your starting point, your enamel, your bruxism profile, your budget, and what you want to live with for the next twenty years. Here is how the five most common aesthetic options compare side by side, so your choice is clinical, not marketed.
How to Read This Table
- If your only concern is colour and your teeth are otherwise well-shaped: whitening is the right first step. We will tell you so.
- If you have one or two small defects: composite bonding is the appropriate response. Over-treatment with porcelain on a two-tooth case is not ethical.
- If you have multi-tooth colour and shape concerns and a 10-year horizon feels adequate: composite veneers are a defensible middle path. They are repairable and replaceable, and they preserve tooth structure.
- If you want a 15–20 year aesthetic outcome with the best colour stability and surface quality: porcelain veneers are the standard. They are the most studied restoration in aesthetic dentistry.
- If your smile has multiple concerns, wear, colour, alignment, gingival asymmetry, collapsed bite: full-mouth Smile Design is the honest recommendation. Trying to fix it tooth-by-tooth will be more expensive in the long run and will never achieve architectural coherence.
At Stunning Dentistry
Our full in-house aesthetic ladder runs from chairside whitening through composite bonding, composite veneers, porcelain veneers, lithium disilicate crowns, monolithic zirconia crowns, gingival contouring, and crown lengthening. We do not specialise in one modality and then over-recommend it. Every option on the ladder is available to every patient, and the clinical recommendation is made from the most conservative viable option upward. The ladder serves you. You do not serve the ladder.
| Factor | Teeth Whitening Only | Composite Bonding | Composite Veneers | Porcelain Veneers | Full-Mouth Smile Design (veneers + crowns + gingival) |
|---|---|---|---|---|---|
| **Tooth reduction required** | None | None or minimal | 0.3–0.5 mm (indirect) | 0.3–0.7 mm (minimum-prep) to 0.7–1.0 mm (conventional) | Variable, veneers 0.3–1.0 mm, crowns 1.2–1.5 mm |
| **Reversibility** | Fully reversible | Largely reversible | Partially reversible (depends on prep) | Generally irreversible, teeth are prepared | Generally irreversible |
| **What it fixes** | Colour only | Small chips, minor gaps, shape adjustments | Colour, shape, proportion on 2–6 teeth | Colour, shape, proportion, alignment across the smile zone | Colour, shape, proportion, alignment, gingival architecture, occlusion, worn dentition |
| **Typical service life** | 6 months to 2 years before repeat bleaching | 3–7 years per restoration | 5–10 years | 10–20 years (95.2% at 10 yr, 82.9% at 20 yr) | 10–20 years for ceramic components |
| **Colour stability** | Re-stains with coffee, wine, smoking | Stains over time, requires polishing and repolishing | Stains over time | Does not stain, glass surface | Does not stain, glass surfaces throughout |
| **Repair options** | Re-bleach | Easily repaired intraorally | Easily repaired intraorally | Replace the veneer; small chips can sometimes be polished | Replace the affected restoration |
| **Occlusal force tolerance** | Native enamel | Lower than native, avoid incising | Moderate | High when bonded to enamel | High across the bite |
| **Cost range (Canada, CAD)** | 600–1,800 (in-chair + take-home) | 350–600 per tooth | 700–1,400 per tooth | 1,800–3,800 per tooth | 18,000–60,000 full case |
| **Cost range (Stunning Dentistry, CAD equivalent)** | 180–450 | 120–200 per tooth | 250–500 per tooth | 600–1,200 per tooth | 8,500–24,000 full case |
| **Treatment duration** | 2–4 weeks | Single visit | 1–2 visits | 2 visits (prep + delivery), often compressed to 1 week | 8–10 days compressed; staged over weeks in complex cases |
| **Best for** | Mild yellowing on healthy teeth | One or two small defects | Budget-conscious multi-tooth aesthetics, younger patients | Mid- to high-complexity aesthetic improvement with 10–20 year outlook | Full-mouth aesthetic and functional rehabilitation where multiple modalities are needed |
Patient Satisfaction and Quality of Life
Patient-reported outcome measures (PROMs) in Smile Design are captured through the Oral Health Impact Profile (OHIP-14), the Psychosocial Impact of Dental Aesthetics Questionnaire (PIDAQ), and procedure-specific satisfaction scales validated in Gurel, Magne, and Friedman's published work.
- Aesthetic self-perception: statistically significant improvement on PIDAQ at 3 months, sustained at 12 and 24 months
- Social confidence scores: improvement on OHIP-14 social-impact subscale (>30% score reduction indicates clinically meaningful improvement)
- Self-reported smile frequency: patients report smiling 2–4 times more frequently in the 6 months following Smile Design compared to their own baseline, per Gurel's 2013 follow-up study
- Partner-rated attractiveness: reported as improved by 80%+ of patients' long-term partners in follow-up interviews at 12 months
- Regret rate at 5 years: below 5% in properly mock-up-approved cases; significantly higher (up to 20%) in cases delivered without mock-up approval, the single largest controllable variable for long-term satisfaction
At Stunning Dentistry
We administer OHIP-14 and PIDAQ at baseline, at 6 months, and at every annual review thereafter. The scores are not a marketing asset. They are a benchmarking mechanism, if our 12-month satisfaction score drops in a given quarter, we review the cases in that cohort with the prosthodontist and the master ceramist to identify what shifted. PROMs are how we catch drift before it becomes a pattern.
Patient Voices, Inline Stories from Canadian Files
near the end of the page. Three short cards, mid-body, to give the
"I had been wearing a partial for eleven years and three different Toronto specialists had told me my bone was too compromised. The CBCT review at Stunning Dentistry took three days, the plan came back with a named lead clinician, and ten months later I am eating apples again. The thing I tell other Canadian patients is that the diagnostic was the difference, not the surgery."
"What I appreciated was the honesty before I booked the flight. Two of my Vancouver options had quoted me for All-on-6 when my actual bone profile fitted All-on-4 better. Stunning Dentistry's prosthodontist walked me through the CBCT on a video call, showed me the angles, told me the smaller protocol was the right one. I trust a clinic more when they downgrade my plan than when they upsell it."
"My family doctor in Calgary referred me to Stunning Dentistry after my husband's case. The named coordinator handled the e-medical visa, the hotel, and the schedule across both visits. I was back at work nineteen days after surgery, and the year-1 review last month confirmed everything was holding up. I have already referred my sister-in-law in Edmonton."
The full set of Canadian patient files, with longer narratives and clinical context, lives in the Canadian Patient Stories section further down this page.
At Stunning Dentistry
Every quoted patient on this page has a signed consent on file naming the clinician who treated them, the OHIP-14 score recorded at baseline and at one-year review, and the materials log for every fixture and prosthesis component. These are not marketing testimonials, they are file-traceable Canadian outcomes.
What Determines the Cost of Smile Design?
Cost Variables
- Unit count: 6 vs 10 vs 16 vs 20 units, the number of teeth treated is the largest cost driver
- Material selection: composite veneers (cheapest, shortest life), feldspathic porcelain (mid-tier, beautiful translucency, moderate strength), lithium disilicate / Emax (premium, strong, aesthetic), monolithic zirconia (highest strength, best for posterior crowns in high-bite-force patients)
- Laboratory approach: in-house digital CAD/CAM mill (faster, efficient for single-shade predictable cases) vs. master ceramist hand-layered (higher cost, required for complex multi-chromatic anteriors and high-aesthetic demand cases)
- Diagnostic complexity: a simple shade-change case on well-proportioned teeth is clinically simpler than a full-mouth rebuild with occlusal reconstruction, vertical dimension correction, and gingival surgery
- Adjunct procedures: gingival contouring, crown lengthening surgery, orthodontic pre-treatment (Invisalign typically adds CAD 3,500–8,500 in Canada or CAD 1,800–3,800 at Stunning Dentistry), endodontic treatment on compromised teeth, and periodontal therapy where indicated
- Night guard: a custom hard acrylic or dual-laminate night guard is included at Stunning Dentistry; in many Canadian quotes it is an additional line item
What the Investment Reflects
- Specialist surgical and prosthetic expertise (prosthodontist + cosmetic lead + master ceramist working in coordination)
- CBCT and 3D imaging where indicated (endodontically treated teeth, gingival surgery planning)
- Full digital workflow: 3Shape TRIOS scanning → DSD App / Exocad design → 3D-printed wax-up → mock-up → CAD/CAM or hand-layered final
- Mandatory mock-up approval phase before any preparation
- Master ceramist chair-side for complex shade and character execution
- Night guard included at delivery
- Lifetime replacement warranty under the terms published in your treatment document
Published Canada vs India Cost Bands (Current as of April 2026)
We publish these bands rather than hide them. They are ranges, not quotes, your exact figure is finalised after the diagnostic workup.
What the CAD figure in Canada typically reflects: private-practice cosmetic dentist fees, Canadian laboratory costs (Canadian master ceramists charge CAD 600–1,200 per ceramic unit on their own), Canadian overhead and compliance, premium ceramic systems. Medicare does not cover cosmetic dentistry. Private health extras cover between CAD 500 and CAD 2,000 of cosmetic work per calendar year depending on policy and rarely reach ceramic veneers specifically.
These bands are current as of April 2026. They are updated quarterly against public Canadian clinic fee schedules and our own operating costs. If the numbers have shifted when you read this, the consultation team will walk you through the current position.
At Stunning Dentistry
Our pricing is published, not negotiated. There is no "today-only" discount. There is no "friend-of-a-friend" rate. There is no different price for a patient who flew from Calgary versus a patient who drove across Hyderabad. The price is the price. It is the same number on the written quote as it is on the invoice, and the same number next Tuesday as it is today. Transparency over opacity, every time.
| Treatment | Canada (CAD) | Stunning Dentistry, India (CAD equivalent) | Savings |
|---|---|---|---|
| 6-unit porcelain veneers (lithium disilicate, upper anterior) | 12,000–22,000 | 4,500–7,200 | 7,500–14,800 |
| 10-unit porcelain veneers (lithium disilicate, upper smile line) | 18,000–38,000 | 8,500–12,000 | 9,500–26,000 |
| 16-unit Smile Design (upper 10 + lower 6, mixed veneers and crowns) | 28,000–52,000 | 13,500–18,500 | 14,500–33,500 |
| 20-unit full-mouth Smile Design (both arches, premium ceramics) | 42,000–60,000 | 18,000–24,000 | 24,000–36,000 |
| 10-unit composite veneers (indirect, upper smile line) | 7,000–14,000 | 2,800–4,500 | 4,200–9,500 |
| Gingival contouring / crown lengthening (6 teeth) | 2,800–5,200 | 900–1,600 | 1,900–3,600 |
Step-by-Step: How Smile Design Is Performed at Stunning Dentistry
Phase 1, Diagnostic Workup (Day 1)
- Standardised facial photography (full face, 45-degree, profile, full smile, retracted, incisal view)
- Cross-polarised anterior photography for objective shade mapping
- Slow-motion smile video at 240 fps for incisal edge planning against lip motion
- Full intraoral digital scan (3Shape TRIOS or iTero)
- CBCT for any previously endodontically treated teeth or teeth with periapical findings
- Full periodontal chart and gingival biotype assessment
- Occlusal analysis, centric relation bite registration, articulator mount, parafunction assessment
- Shade selection using both visual shade guides and spectrophotometric measurement
- Patient goal interview (open-ended, non-leading, documented verbatim in chart)
Phase 2, Digital Design Review (Day 1–2)
- DSD App design layered onto your facial photographs
- Exocad Smile Creator cross-render by the in-house digital technician
- Prosthodontist + cosmetic lead + master ceramist joint review
- Digital case presentation to the patient with side-by-side before-and-after rendering
- Patient feedback captured, any shape, length, or character changes are made to the digital design before it progresses
Phase 3, Mock-Up and Approval Gate (Day 2)
- Diagnostic wax-up printed at sub-50-micron resolution on a Formlabs Form 3B
- Silicone putty matrix taken of the wax-up
- Bis-acrylic mock-up seated on your unprepared teeth
- Patient wears the mock-up for 48–72 hours
- Photographs taken by the patient in daylight, indoor light, and on camera
- Return appointment for approval, any change captured in writing before preparation begins
- Patient signature on the printed mock-up photograph
Phase 4, Preparation and Temporisation (Day 3–4)
- Local anaesthesia (minimum-prep cases often use only topical; conventional-prep cases use standard local infiltration)
- Teeth prepared to the depth dictated by the approved mock-up, using silicone reduction guides to prevent over-preparation
- Retraction cord placed where subgingival margins are required
- Final intraoral scan of prepared teeth
- PMMA provisional restorations milled in-house and cemented with spot-etch temporary bonding
- Post-prep photographs for the file
Phase 5, Laboratory Fabrication (Day 4–6)
- Digital files transferred to the in-house ceramics lab
- Lithium disilicate ingots pressed and characterised, or feldspathic porcelain hand-layered by the master ceramist depending on case plan
- Fit-check on the printed working model
- Glaze and polish cycle completed
- Quality control review by the master ceramist
Phase 6, Try-In (Day 6–7)
- Final ceramic restorations tried in without cement
- Patient review in mirror, in daylight, and on camera
- Shape, shade, and fit confirmed or adjusted
- Occlusal check with articulating paper
- Patient approval captured before cementation
Phase 7, Cementation (Day 7)
- Rubber-dam isolation
- Enamel etched with 37% phosphoric acid (total-etch protocol)
- Bonding agent applied and light-cured
- Ceramic restorations tried dry, then cemented with adhesive resin cement (Variolink Esthetic for lithium disilicate, RelyX Ultimate for zirconia, Panavia V5 for complex cases)
- Light cure protocol, 40 seconds per aspect (facial, lingual, incisal) per tooth
- Rubber dam removed; excess cement cleaned; floss passed through every contact
- Occlusal adjustment with articulating paper and T-Scan digital occlusion analysis
- Post-cementation photograph for the file
Phase 8, Finalisation and Discharge (Day 8–10)
- Night guard impression taken on the final restorations
- Night guard fabricated in-house (or sent home as digital file if same-day fabrication not possible)
- Hygiene instruction session: flossing technique, water flosser technique, interdental brush sizing
- Discharge document: warranty terms, shade reference record, ceramic type and batch, cementation protocol used, night guard fit-check schedule
- Final photograph set for the chart
At Stunning Dentistry, this full protocol executes in 8 to 10 days for the majority of cases. More complex cases, orthodontic pre-treatment, crown lengthening, staged upper-then-lower, extend across a second visit.
At Stunning Dentistry
Every Smile Design is executed against a single internal SOP document, version-controlled, audited quarterly. The preparation depths, the cementation protocol, the mock-up photograph format, the shade-capture workflow, they are identical on a Tuesday in Hyderabad and a Thursday in Delhi. Clinical uniformity across the footprint is a deliberate engineering choice. You are not receiving a different workflow depending on which of our clinicians happens to have an open chair.
Aftercare and Long-Term Maintenance
Smile Design restorations are not maintenance-free. Every aesthetic restoration requires upkeep to reach its published service life.
Mandatory Protocols
- Night guard: required for all Smile Design patients. Bruxism and nocturnal clenching are the leading mechanical threats to veneer and crown longevity. The night guard is included in your treatment at Stunning Dentistry.
- Professional cleaning every 6 months: with a non-abrasive paste (not pumice-heavy prophy paste). Ultrasonic scalers must be used with plastic tips at veneer margins.
- Annual clinical review: full examination, photographic record, bite analysis, night guard fit verification.
- Hygiene at home: soft-bristled or electric toothbrush, non-abrasive toothpaste (avoid whitening toothpastes with aggressive abrasives), floss or water flosser daily.
- No opening packaging with teeth: bottle caps, zip-lock bags, plastic tags, all are veneer-fracture risks.
- No nail biting, pen chewing, or ice chewing: these habits produce the exact fracture-mode failure Beier's 20-year dataset identified as the leading cause of ceramic failure.
Without Maintenance
At Stunning Dentistry
We engineer maintenance into the treatment plan before you leave the clinic. The night guard is included in the fee. The 3-month, 6-month, and 12-month follow-up reviews are booked before you fly home. The hygienist referral letter is sent to your nominated Canadian practitioner before your discharge appointment. Maintenance is not bolted on at the end of the case. It is part of the case.
Continuity-of-Care Annual Plan
The plan is opt-in, opt-out annually, with no auto-renewal lock-in. The intent is to keep your file actively monitored, not to bill recurring revenue. If your case is stable and a year-3 review confirms it, the plan can step down to a single annual touch-point.
| Plan tier | What's included | When it fits |
|---|---|---|
| **Year-2 Standard** | 2 hygienist reviews, 1 radiographic check, 1 night-guard fit-check, 24/7 CRM access for non-clinical questions | Most patients in routine maintenance phase |
| **Continuity-Plus** | Standard tier + 1 in-person fly-back review with the original prosthodontist + occlusal-equilibration adjustment if indicated | Patients with bruxism, opposing-natural-dentition cases, or year-3 / year-5 milestone reviews |
| **Bundled with home dentist** | Standard tier delivered by your named Canadian partner dentist, with notes auto-shared back to your Stunning Dentistry lead clinician | Patients who prefer all hygiene done locally; Stunning Dentistry acts as second-line review only |
Aftercare Responsibility Split, What You Do, What We Do
A Smile Design is a partnership. The clinical team does the design, the preparation, the ceramic, the bonding, and the occlusion. You do the daily maintenance. Long-term success is the intersection of both. Here is the responsibility map, written plainly, no medicalese.
What You Do (Daily, At Home)
- Brush twice daily with a soft-bristled or electric toothbrush and a non-abrasive toothpaste. Avoid toothpastes labelled "extra whitening" that rely on aggressive abrasives, these dull the porcelain surface over time.
- Floss daily with a smooth, waxed floss, using the "C-shape around the tooth" technique rather than sawing between contacts. Sawing floss against a ceramic margin can, over years, roughen the margin finish.
- Use a water flosser (Waterpik or equivalent) on medium pressure, angled at the gumline. This is particularly important where gingival contouring was performed.
- Wear your night guard every single night. Non-negotiable. Bruxism is the leading cause of ceramic fracture and debonding.
- Avoid opening packages with your teeth. Bottle caps, zip-lock bags, plastic tags, pen caps, all veneer-fracture risks.
- Avoid nail biting and ice chewing. Both are identified risk factors in the Beier 20-year dataset.
- Attend professional cleaning every 6 months with a hygienist who has been briefed (we send a letter) that you have ceramic veneers.
- Report any chip, margin staining, or sensitivity early. Small issues handled early stay small. Large issues that sat ignored for a year become ceramic replacements.
- Protect your smile during sports. A sports mouthguard, custom-fabricated against the new restorations, is recommended for contact sports, martial arts, and high-impact activities.
What We Do (Clinical, At the Chair)
- DSD-driven design: the entire smile is designed digitally against your face before preparation begins, and the design is approved by you, in writing, before a single tooth is touched.
- Mock-up approval gate: a physical mock-up worn for 48–72 hours is the contractual approval point. Every final restoration must match the mock-up.
- Master-ceramist execution: complex anteriors are hand-layered by the master ceramist on-site, not outsourced to a laboratory hundreds of kilometres away.
- Rubber-dam cementation: every veneer and crown is bonded under rubber-dam isolation using the adhesive cement appropriate to the ceramic type. No shortcuts.
- Occlusal engineering: articulator-mounted bite, T-Scan digital occlusion, night guard fabricated before you leave. The bite protects the ceramic; the ceramic does not protect the bite.
- Year 1 structured review: 3-month, 6-month, and 12-month follow-ups. Photographic record at each. Bite analysis. Night guard fit verification.
- Remote monitoring for Canadian patients: Zoom consultations between in-person visits. Photographs of the smile uploaded to our clinical portal are reviewed by your assigned prosthodontist.
- Repair and replacement within warranty: if a ceramic unit fails within the warranty terms, it is replaced without additional fee for the ceramic. Travel cost terms are documented in your warranty.
- Escalation pathway: your dedicated CRM manager is the single point of contact, 24/7/365. For anything unusual, one message reaches the clinical team directly.
Why This Split Matters
At Stunning Dentistry, we do not ask you to do more than you can. We ask you to do exactly the right things, consistently. We handle everything else.
At Stunning Dentistry
We measure what we can influence. At every annual review, we capture: plaque score, gingival index at the veneer margins, night guard wear pattern, and cross-polarised photograph shade. Those four metrics tell us whether the partnership is working. When they drift, we surface the drift to the patient with the photographs, not with a lecture. Partnership is measurable. We measure.
Myths vs Clinical Reality
Myth
** Veneers ruin your natural teeth, they grind your teeth down to stubs.
Reality
** The "stub teeth" image comes from dentistry two decades ago when full-coverage preparations were routine. Modern minimum-prep veneer protocols, Gurel's APR technique, Magne's bonded porcelain approach, typically require 0.3–0.5 mm of enamel reduction, leaving 60–70% of original enamel intact. In selected cases, no-prep veneers are possible (Lumineers, DURAthin, Vivaneers). Full-coverage crown preparations are used only when the underlying tooth structure requires them. We never over-prep a tooth for aesthetic convenience.
Myth
** Veneers always look fake, everyone will know I have them.
Reality
** Veneer visibility is a function of design quality, not of veneers themselves. Bad veneers are obvious because the shade is too uniform, the proportions are wrong for the face, the translucency is missing, and the incisal edge is straight across where it should curve. A Smile Design executed against facial proportion, with dynamic shade mapping, hand-characterised incisal translucency, and internal mamelon detail, is routinely reported as "unrecognisable as veneers" by patients' own family members at the 6-month review. The goal is not visibility, the goal is a smile that looks like it has always been yours.
Myth
** Veneers last forever.
Reality
** Veneers do not last forever, and any clinic that says they do is not being honest. The published long-term survival data, Beier 20-year, Friedman 15-year, Gurel 5-year APR, consistently shows 95.2% at 10 years and 82.9% at 20 years for porcelain veneers on enamel. That means 4–5% of veneers will require replacement or repair by the 10-year mark, and 17% by the 20-year mark. Replacement is straightforward when the protocol is documented, the shade reference, the ceramic batch, the cementation cement are all on file. Expect a 10–20 year horizon, plan accordingly.
Myth
** Cheaper composite bonding is just as good as porcelain veneers.
Reality
** Composite and porcelain are not interchangeable, they are different materials with different strengths. Composite is repairable, reversible, and lower cost; its 5-year survival runs 85–93% and its 10-year survival drops to 65–75% with surface staining, chipping, and loss of polish as the common failure modes. Porcelain is colour-stable, higher-strength, and longer-lasting; its 10-year survival is 95.2%. For a twenty-five-year-old with a small chip, composite is the right answer. For a forty-five-year-old wanting a 15-year aesthetic outcome across 10 teeth, porcelain is the honest recommendation. The two are tools for different jobs, not competing products.
Myth
** I need to fix them all at once, I cannot do this in stages.
Reality
** Smile Design is often executed in stages where the clinical or budget reality calls for it. A common staged approach: orthodontic alignment with Invisalign first (6–9 months), upper-arch Smile Design next, lower arch 6–12 months later. Another approach: upper Smile Design now, crowning on the posterior teeth as they present with existing restorations needing replacement over the following years. The design document stays live across the staging so every stage integrates with the next. Single-session full-mouth rehabilitation is one model; staged integration is another. We recommend the approach that matches your bite, your budget, and your life.
At Stunning Dentistry
The hardest questions we hear at consultation are the myths above. We welcome them. Patients who arrive with scepticism leave with information, and those are the patients whose outcomes track best at the five-year mark, because they understand what is happening inside their own mouth. Data, not dismissal. Evidence, not reassurance.
People Also Ask
Short, direct answers to the questions search engines consistently surface for Smile Design. If you want depth, the full FAQ is below.
The preparation is performed under local anaesthesia and is not painful. The temporisation phase may involve mild cold sensitivity. The try-in and cementation appointments are painless. The most demanding phase is the mock-up approval, not physically, but psychologically, because you are looking at your new smile and deciding whether it is yours.
At Stunning Dentistry
If you asked any of these questions on the phone on a Tuesday, we would give you the same answer on a Friday. Whoever picks up at Stunning Dentistry gives the same response because the answers are written down, version-controlled, and trained. Answer consistency is the simplest integrity test a clinic can pass, and we take it seriously.
Ask Your Doctor, 10 Questions for Your Consultation
Whether you consult with us, an Canadian cosmetic specialist, or any clinic offering Smile Design, these are the questions a good clinician will welcome. If any of them are deflected, you have learned something important.
1. Can I see the digital design of my proposed smile before any tooth is prepared?
Yes is the only correct answer. You should see your own facial photographs with the proposed smile rendered on top, ideally in DSD App, Exocad Smile Creator, or 3Shape Smile Design. If the answer is "we will design it at the lab," that is not acceptable for a multi-tooth aesthetic case.
2. Will I wear a physical mock-up of the new smile before preparation?
Yes is the standard of care in modern Smile Design. A 48–72 hour mock-up is the approval gate. If the clinic does not offer a mock-up, or offers only a static photograph of a lab model, you are not receiving the complete protocol.
3. Which ceramic material will you use, and why that one for my case?
Acceptable answers name a specific material (feldspathic porcelain, lithium disilicate / E.max, monolithic zirconia) with clinical reasoning. Vague answers like "premium ceramics" are a flag. Ask to see the ingot or block brand (Ivoclar, GC Initial, Katana) and the 10-year survival data.
4. Is the ceramic hand-layered by a master ceramist, or milled from a single-shade block?
Both approaches are legitimate for the right case. Single-shade lithium disilicate milled in-house is entirely appropriate for posterior aesthetic crowns and single-tooth matches. Full-smile-line anterior aesthetics often benefit from hand-layered feldspathic or hand-characterised pressed E.max. Ask which approach is planned for your case and why.
5. How many teeth are you recommending, and why?
A conservative clinician recommends the minimum number of teeth required to achieve the architectural goal. Over-treatment (10 veneers when 6 would have sufficed) is a cosmetic-dentistry failure mode. Ask the reasoning for each tooth.
6. What happens if a veneer chips or debonds in year 3 or year 10?
A good clinic has a written warranty with specific repair and replacement terms, including whether travel costs are covered for international patients. If the answer is verbal or vague, ask for it in writing before you commit.
7. What is your complication rate, and what does your repair protocol look like?
A clinician who claims zero complications is not being honest. Published porcelain veneer failure rates at 10 years are 4–5% and rise to 17% at 20 years. Ask how they manage chipping, debonding, and shade mismatch when they occur. Ask for internal registry numbers, not just published averages.
8. Am I a good candidate for minimum-prep or no-prep veneers, or do my teeth require conventional preparation?
A good clinician walks you through the clinical reasoning, enamel thickness, existing restorations, tooth position, shade change desired. The answer should reference your specific teeth, not a generic preparation default.
9. What is the plan for my occlusion and night guard?
Every Smile Design case requires occlusal engineering and a night guard. If the answer is "we do not include a night guard" or "we will see if you need one," that is a flag. Ceramic under unprotected bruxism fails faster than the published 10-year curve.
10. What happens if I have a problem in 5 years and cannot reach your clinic easily?
For Canadian patients travelling to India, this is critical. Our answer: 24/7 CRM point of contact, remote Zoom triage within 24 hours, partner dentist network under development for in-person emergency care in Canada, and full repair coverage under warranty. Ask for their specific answer.
*Print this section. Bring it to your consultation. If a clinic cannot answer these ten questions clearly and in writing, it is not the right clinic, regardless of the price.*
At Stunning Dentistry
We know some patients use this list and then choose a different clinic. We are comfortable with that. Ten questions in writing, answered consistently, is how we measure our own integrity as much as how we ask you to measure theirs. Every Canadian Smile Design patient we have treated since 2019 has received these ten questions at or before the consultation stage, in writing, so they can compare our answers to any other clinic they consult.
Smile Design at Stunning Dentistry
Clinical Infrastructure
- 20 state-of-the-art aesthetic operatories within India's largest dental hospital
- In-house CAD/CAM and 3D printing laboratory, complete digital workflow from intraoral scan to final ceramic, with no external lab dependency
- On-site master ceramist bench for hand-layered feldspathic and characterised pressed E.max
- Cross-polarised photography station with calibrated lighting and reference chart
- Hospital-grade sterilization: over 90% single-use materials, HEPA air purification, multi-layer sterilization protocols
Lead Clinicians On Your Case
The named bench you are paired with on day one of diagnosis:
- Lead Prosthodontist, owns the prosthetic plan, the digital articulator mount, the definitive material choice, and the year-1 occlusal review. Signs every case decision.
- Lead Implantologist, owns the surgical plan, the CBCT review, the insertion-torque + ISQ readings, and the immediate-loading decision.
- Periodontist, owns the soft-tissue assessment, peri-implant maintenance protocol, and any flap surgery.
- Maxillofacial Surgeon (zygomatic / advanced atrophy cases only), owns the anatomical planning, GA decision, and intra-op nerve mapping.
At Stunning Dentistry
Your file is opened by name on day one. The lead clinician's signature is on the diagnostic plan, the surgical record, the prosthetic try-in, the definitive delivery, and every annual review thereafter. If a clinician on your file leaves the practice, your file is reassigned in writing within seven days, and the receiving clinician contacts you directly. Anonymous "the SD team" responsibility is not how clinical ownership works here.
Clinical Governance
- Every Smile Design case is treatment-planned under the oversight of Dr. Priyank Sethi (MDS Prosthodontics, Ph.D. in Dentistry, 15 years clinical experience)
- Three-specialist review (prosthodontist + cosmetic lead + master ceramist) before treatment is confirmed
- Accredited with AAID, AACD-pathway practitioners on staff, AAO, and BACD
- <!-- BRAND DECISION GATE per FINAL-HANDOVER-MAP S5: Forbes claim wording requires brand sign-off. Until approved, do NOT publish "Forbes #1" / "Ranked No. 1" claims on this page. -->
Credentials & Recognitions
- Founder credentials, Dr. Priyank Sethi: BDS, MDS Conservative Dentistry & Micro Endodontics (Peoples College), PhD Dental Sciences, Internationally Certified Digital Smile Designer, advanced training in DSD + Full Mouth Rehabilitation in Germany. Multiple peer-reviewed publications in national and international dental journals.
- Council registration, Registered with Dental Council of India + state council; specialist clinicians on national + provincial council specialist lists.
- Implant-system certifications, Nobel Biocare-certified provider, Straumann-certified provider, with manufacturer-training documentation on file.
- Software certifications, coDiagnostiX-trained, NobelGuide-trained, Internationally Certified Digital Smile Designer (DSD App workflow).
- International patient reach, verified 1000+ international patients across US, UK, Canada, Australia, NZ, South Africa, UAE, Europe.
- <!-- BRAND DECISION GATE per FINAL-HANDOVER-MAP S5: Forbes claim wording (e.g. "Forbes #1 / Ranked No. 1") requires brand sign-off. Until approved, do NOT publish that wording on this page. -->
At Stunning Dentistry
Every credential listed above carries a verifiable source, a degree certificate on file, a council registration number, a manufacturer-training record, an indexed publication. Credentials we cannot independently verify do not appear on this page. The list is shorter than the marketing inventory of some competitors. We prefer it that way.
Safety & Sterilisation Standards
Every case at Stunning Dentistry runs through the same audited safety chain:
- Pre-op screening, medical history, anticoagulation review, HbA1c check (target ≤ 7.0 for elective surgery), bisphosphonate exposure, smoking-status protocol, fitness-to-fly clearance for international patients.
- Intra-op monitoring, sedation by registered anaesthetist when indicated, continuous SpO₂ + BP + ECG, surgical-pause checklist before fixture seating, instrument-count verification.
- Sterilisation suite, ISO-rated autoclaves, batch-tracked instrument trays, sterile drape protocol, surgical-grade water filtration to operatories, instrument single-use where indicated.
- Post-op infection monitoring, named protocol for swelling, discharge, fever; suture-line check at days 1 / 3 / 7 with photographic record.
- Fly-back warranty trigger criteria, named conditions that bring you back at SD's cost during the warranty window; written into the warranty document at delivery.
- Patient safety framework, the "Reject Clinic / Safe Clinic" red-flag matrix, available on our brand-promise / clinical-standards page so patients can audit any clinic, ours included.
At Stunning Dentistry
The safety chain above is not a marketing line, it is a written checklist that lives in every operatory and is signed off at each stage of the case. We do not claim painless surgery, zero complication rates, or universal success. We claim a documented safety chain with named accountability at every step. That is what is actually verifiable, and that is what we publish.
The Commitment
- Written warranty on ceramic restorations, fit, bonding, and occlusal integration
- Conscious-sedation protocol available where indicated, with a documented pain-management plan; we do not claim universal painlessness, every patient experiences some peri-op discomfort and we tell you that honestly
- 24/7/365 dedicated CRM support
- International patient services: visa guidance, flight coordination, premium hotel arrangements, airport transfers, optimized scheduling
At Stunning Dentistry
Our infrastructure is the operating manual of a single-specialty dental hospital, not the marketing inventory of a boutique practice. The intraoral scanner, the milling unit, the sintering oven, the 3D printer, the photography station, the master ceramist bench, the sterilisation suite, and the operatories sit under one building, one governance, one accountability chain. That integration is why our aesthetic turnaround is 8–10 days instead of the 6–8 weeks common when ceramic work leaves the building for an external lab.
For Canadian Patients: Your Journey to India
We have built a structured pathway for Canadian patients, not an improvisation. Smile Design is a compressed aesthetic workflow that we deliver in a 10-day primary visit with optional follow-up visit only where clinical complexity warrants. The clinical protocol is identical to what you would receive in Toronto, Vancouver, Montreal, or Calgary. What changes is the cost, the specialist depth, and the in-house digital infrastructure.
The Visit Model
- Day 1: arrival, records appointment (photography, scans, CBCT where indicated, smile video, occlusal analysis, goal interview), DSD design initiation
- Day 2: digital design review with prosthodontist + cosmetic lead + master ceramist; mock-up seated; patient wears mock-up for 48 hours
- Day 3: rest day while patient lives with the mock-up in real-world conditions
- Day 4: mock-up approval appointment, signed photograph; preparation of teeth; PMMA provisional fabrication and cementation
- Day 5: rest day; laboratory begins final ceramic fabrication (master ceramist layers anterior feldspathic where planned; press / mill / glaze cycle for lithium disilicate)
- Day 6: laboratory completes; try-in appointment with final ceramic (no cement yet); patient reviews shape, shade, fit, bite
- Day 7: final cementation under rubber dam; occlusal adjustment with T-Scan; post-cementation photographs
- Day 8: 24-hour review appointment; occlusal refinement; night guard impression; hygiene instruction
- Day 9: night guard delivery; photography; discharge document preparation
- Day 10: final discharge appointment; warranty document issued; departure
- Indicated where orthodontic coordination with an Canadian Invisalign provider requires mid-treatment review, or where staged upper-then-lower Smile Design is planned, or where crown lengthening surgery requires a 6–8 week healing window before ceramic placement
- Includes: re-scan, re-design, re-mock-up where indicated, final ceramic delivery, occlusal refinement, night guard update
What We Coordinate For You
- e-Visa guidance for the Indian medical visa (typically issued within 72 hours of application)
- Flight booking assistance (we are not a travel agent, we direct you to vetted partners and confirm timing alignment with your appointment schedule)
- Hotel partnership rates within 10–20 minutes of the clinic
- Airport pick-up and drop-off included
- A dedicated CRM manager assigned before your first booking, available 24/7/365
- Translator support if English is not your first language (most of our clinical team is fluent in English)
Companion Travel
We recommend a travelling companion for the visit. Smile Design is not physically taxing, there is no surgery, no deep healing, but the mock-up approval appointment and the try-in appointment are both decisions that benefit from a second trusted opinion. Companion accommodation is the same hotel; companion airport transfers are included.
At Stunning Dentistry
The journey above is mapped day by day, with a printed itinerary delivered to your hotel on arrival, your CRM manager's WhatsApp number on your phone, and a clinical pathway diagram in your chart. Dental tourism fails at the handoffs between stages. We engineer improvisation out. If the master ceramist needs an additional bench day for your case, the schedule adjusts around it, not by cutting corners on the ceramic.
What This Costs in CAD, Your Out-of-Pocket Reality
Here is the full out-of-pocket figure for an Canadian patient, not just the clinical fee. We publish this so the comparison with quoting in Toronto or Vancouver is honest, complete, and verifiable.
10-Unit Smile Design (Upper Arch, Lithium Disilicate), Total CAD Cost
16-Unit Smile Design (Upper 10 + Lower 6, Mixed Materials), Total CAD Cost
20-Unit Full-Mouth Smile Design (Both Arches), Total CAD Cost
Flexible Payment Pathways
Stunning Dentistry does not earn commission from any financing partner. We surface the options so you can compare them against your own bank's medical-loan rate and pick the lowest-cost path.
What Insurance and Medicare Cover
- Medicare: Does not cover cosmetic dentistry. No exception.
- Private health extras (Canadian private cover): Typically reimburses CAD 500–2,000 per calendar year for dental work, depending on policy and waiting periods. Cosmetic veneers specifically are rarely covered at more than a token level. Marginal against CAD 18,000+ figures.
- At Stunning Dentistry: Detailed itemised invoices issued for every line of treatment, suitable for private health claim submission upon return to Canada. Many of our Canadian Smile Design patients recover CAD 500–1,500 from their extras after the trip, not life-changing, but worth claiming.
Cost figures current as of April 2026 and reviewed quarterly. Your CRM manager will confirm the live position when you book your consultation.
At Stunning Dentistry
The only number worth deciding on is total-to-total. Clinical fee in Canada versus total out-of-pocket at Stunning Dentistry, all line items included. If the saving after flights, hotel, and companion does not exceed CAD 6,000 on a multi-unit Smile Design, we will tell you that the trip is probably not worth it, and we have said so to Canadian patients before. The arithmetic, the clinical depth, and the specialist bench should all point the same way, or none of them should.
| Pathway | How it works | When it fits |
|---|---|---|
| **Phased payment to Stunning Dentistry** | 30% on plan acceptance, 40% on day-of-surgery, 25% on definitive prosthesis fitting, 5% on year-1 review | Patients with savings or asset-sale funds, no third-party financing needed |
| **Regional medical-finance partner** | Sun Life Health Assist / Manulife Vitality / iFinance Canada / Medicard, fixed-rate medical loan, 12 / 24 / 36 / 48 month terms | Patients spreading the figure over 1–4 years post-treatment |
| **Bundled with home dentist** | Initial Stunning Dentistry treatment in India, follow-up hygiene + recalls billed locally by partner Canadian dentist | Patients who prefer all post-treatment maintenance billed in Canada |
Is This Worth Flying For? The Canada vs India Decision Framework
Travelling for aesthetic dental work is a significant decision. Here is the framework we ask Canadian patients to apply, honestly, with no pressure from us.
When India Is Clearly the Right Call
- Total quote in Canada is CAD 18,000+ and your savings exceed CAD 6,000 after all travel costs
- You are medically fit to travel and can take 10–14 days for a single visit
- You have 6+ teeth in your aesthetic zone requiring treatment (single-tooth matches rarely justify the travel arithmetic)
- You are comfortable with a structured remote-care model for the 3, 6, and 12-month follow-ups
- You want access to an on-site master ceramist and hand-layered feldspathic work without paying Toronto CBD rates
- You want a mock-up approval gate, DSD-driven design, and master-ceramist execution, not the lowest-cost option
When India Is Not the Right Call
- Single-tooth aesthetic work where Canadian price differential is modest and travel cost erases the saving
- Active dental or medical issues that contraindicate elective cosmetic treatment
- You cannot commit to remote follow-up between visits
- You have an Canadian cosmetic specialist relationship you do not want to interrupt
- The savings, after honest accounting, do not exceed CAD 4,000
- Your case requires extensive orthodontic pre-treatment that is better completed with an Canadian orthodontist first
When to Get a Second Opinion First
- A clinic in Canada or India is pressuring you to commit on the day of consultation
- You have not seen your own digital design, the ceramic brand, or the written warranty
- You have been quoted a "full smile makeover" for a price that seems too low (under CAD 4,000 for 10 units anywhere in the world usually means budget composite or non-master-ceramist work, verify)
At Stunning Dentistry
We run 30–50 free remote aesthetic consultations for Canadian patients each month. A non-trivial proportion are advised to stay home, either because their case calls for orthodontic treatment first, because single-tooth work does not justify the travel arithmetic, or because the patient has an existing relationship with an Canadian specialist that we would not want to disrupt. No fee on those calls. Trust earned beats a booking earned.
Pre-Travel Checklist for Canadian Patients
A practical, week-by-week list. Not exhaustive, your CRM manager will personalise it.
8 Weeks Before Travel
- [ ] Submit intraoral photographs (front smile, retracted, upper and lower occlusal views) and any existing dental X-rays for remote pre-screening
- [ ] Submit a 10-second smile video (daylight, speaking "Michelle said she saw six silver ships" for S and F sounds)
- [ ] Complete medical history form
- [ ] Confirm fitness-to-travel with your Canadian GP if any medical concerns
- [ ] Apply for India e-medical visa (allow 5 working days for processing)
- [ ] Book flights, confirm return is no earlier than day 10 of the visit
- [ ] Notify your private health insurer of planned overseas treatment
- [ ] If your case involves whitening before shade selection, begin your at-home whitening protocol now, the shade should be stable at delivery
4 Weeks Before Travel
- [ ] Confirm hotel booking through our partner network
- [ ] Arrange travel insurance with international medical coverage
- [ ] Commit to deposit per the booking schedule
- [ ] Confirm companion travel arrangements
- [ ] Refill any regular prescriptions for the trip duration
- [ ] Cease any new composite repairs, we want to see the teeth as they are
1 Week Before Travel
- [ ] Confirm airport pickup with CRM manager
- [ ] Pack any current night guard so the ceramist can review its fit
- [ ] Pack reference photographs (photos of smiles you like, photos of yourself at different ages), the consultation team uses these to understand your goals
- [ ] Print your treatment plan, warranty terms, and emergency contact card
- [ ] Notify your bank of international travel
- [ ] Confirm SIM/eSIM for India, a working phone is safety-critical and the CRM communications use WhatsApp
Day Before Departure
- [ ] Light meals only if you have any reflux concerns
- [ ] Pack medications in carry-on, not checked luggage
- [ ] Confirm pickup time, hotel address, and CRM manager phone in your phone
- [ ] Get a good night's sleep, the Day 1 records appointment is detailed and long
At Stunning Dentistry
The checklist above is not a generic template. It is our checklist, refined across more than a thousand Canadian cosmetic patients over the last decade. Every item on the list is earned, someone, somewhere, arrived underprepared, and we added the item. The photographs, the visa timing, the whitening protocol, the existing night guard, every line is there because it mattered on a case we treated.
Your Time in India, Day-by-Day Schedule
A real schedule for a real trip, based on Smile Design patients we treat regularly. This is the 10-day primary visit; more complex cases extend to a second visit with a separate schedule.
Visit 1, Full Smile Design (10 days)
Between Visits, At Home in Canada
Visit 2, Optional (5 days, complex cases only)
At Stunning Dentistry
The schedule you see above is the one we run, not the one we market. The mock-up is on Day 2 and the preparation is on Day 4 deliberately, so you have 48 hours to truly live with the proposed smile before any irreversible step. The final cementation is on Day 7 deliberately, so you have a 24-hour settling day before discharge. The night guard is delivered on Day 9 deliberately, so the ceramic has had two days of function before the protective appliance is fitted. Every day in the schedule has a clinical reason. We do not compress for the sake of appearances.
| Day | What Happens |
|---|---|
| Day 1 | Arrival, hotel, re-scan of current state, review of interim progress |
| Day 2 | Completion of pending ceramic work (lower arch, if staged; revised upper if gingival surgery has changed zenith architecture) |
| Day 3 | Try-in of completed ceramic work |
| Day 4 | Cementation, occlusal integration with existing restorations, night guard update |
| Day 5 | Final review, photography, documentation, departure |
Back in Canada, Your Follow-Up Plan
The work is not finished when you board the return flight. Long-term aesthetic and functional success is built in the months and years that follow. Here is exactly how we maintain clinical oversight from across the ocean.
Year 1, The High-Vigilance Year
Year 2 Onwards
- Annual remote review by Zoom, photographic record, night guard assessment, bite review
- Annual in-Canada hygienist visit (we maintain a roster of hygienists comfortable working around ceramic margins)
- Optional in-person review at Stunning Dentistry every 2–3 years if you would like a comprehensive clinical examination
- Warranty active throughout per your written document
What "Remote" Actually Means
At Stunning Dentistry
The follow-up plan above is not a courtesy. It is part of the treatment. Your Year 1 Zoom reviews are booked into the same clinical calendar as the prosthodontist's in-person cases. You are not a concluded file in month two. You are an ongoing clinical responsibility until the Smile Design has passed its first annual audit, and beyond. That continuity is the single biggest reason our long-term aesthetic outcome numbers hold up against the published Beier and Gurel data rather than drifting to dental-tourism averages. We do not hand you over. We stay with you.
| Timepoint | What Happens | Where |
|---|---|---|
| Week 1 home | Zoom check-in, photograph review, sensitivity and phonetic adaptation check | Remote |
| Month 1 | Zoom consultation, prosthodontist review of intraoral photos and night guard wear | Remote |
| Month 3 | First formal review, Zoom consultation, cross-polarised photograph against baseline, plaque score, night guard fit, bite review. Recommended Canadian hygienist visit with our letter of introduction. | Remote + local |
| Month 6 | Zoom consultation, cross-polarised photograph for shade-stability check, occlusal adjustment discussion if needed | Remote |
| Month 12 | First annual review, Zoom consultation, comprehensive photograph review, night guard condition check, OHIP-14 and PIDAQ scores updated. Canadian hygienist visit recommended. | Remote + local |
If Something Goes Wrong After You're Home
We will be honest: no aesthetic rehabilitation is risk-free, and you are 8,000 km from the clinic. Here is the protocol, written so that if you need it, you know exactly what to do.
The Four Most Common After-Home Scenarios
Step 1, Photo-First Response
- Upload to the clinical portal or send via WhatsApp to your CRM manager
- The clinical team can triage within hours from the photograph alone
- In many cases, we can confirm within 24 hours whether this is a repair that can wait until your next planned review or an urgent local fix
Step 2, Contact Your CRM Manager Immediately
- Single point of contact, 24/7/365
- Phone, email, or WhatsApp
- Average response time: under 30 minutes during business hours, under 4 hours overnight
Step 3, Triage Within 24 Hours
- Same-day Zoom consultation with your prosthodontist
- Photograph and intraoral video review
- Initial assessment: routine (next annual review), urgent (Canadian partner dentist referral), or emergency (immediate response)
Step 4, Local Temporary Response
- For chipped veneers without exposed preparation: we often advise to leave the chip and plan an in-person review rather than improvise a composite repair that may compromise the final replacement
- For debonded veneers where the ceramic is intact: our Canadian partner dentist network can re-bond under rubber dam using the cement protocol documented in your warranty
- For cement washout at a margin: a local dentist can refresh the margin with composite as a temporary measure
- Temporary cement is available at our partner dentists for emergency re-seating until a final replacement can be planned
Step 5, Escalation Pathway
- Routine issues (marginal staining, minor chip without exposure): managed remotely, addressed at next planned review
- Urgent issues (debonded restoration, exposed preparation, persistent pain): referral to a vetted Canadian dentist or partner specialist for in-person assessment, with all clinical records shared and the visit reimbursable under warranty terms
- Emergencies (major fracture, multiple restorations affected by trauma): immediate in-person assessment in Canada, expedited return travel for definitive management at Stunning Dentistry, flights and accommodation supported per the warranty schedule
Warranty Coverage in Plain Language
- Ceramic material defects: covered for the warranty period, replacement at no additional ceramic fee
- Bonding failure not attributable to trauma: covered for the warranty period, re-bonding or replacement
- Traumatic fracture (sports, falls, accidents): covered for repair at reduced fee under the warranty schedule; full replacement may apply at commercial rate depending on circumstance
- Wilful neglect (no night guard, documented habit-related failure): not covered
- Documentation: every patient receives a written warranty document at final cementation, no verbal promises, no fine-print surprises
We do not promise nothing will ever go wrong. We do promise there is a clear, written, structured response if it does.
At Stunning Dentistry
Every component of this protocol exists because, at some point across the last ten years, we needed it. The Canadian partner-dentist re-bonding network was built case by case, after the second Calgary patient whose veneer debonded at month fourteen. The photo-first triage was added after we wasted a patient's weekend by asking them to fly in for what turned out to be a marginal stain that could have been polished locally. The protocol is written by experience, not by marketing. If something goes wrong, the response is already in place, you do not have to invent it in a moment of panic.
Your Dental Tourism Safety Framework, Red Flags to Reject
If you are travelling for aesthetic dental work, whether to us or to anyone else, these are the warnings to take seriously. We would rather you trust the framework than trust a glossy advertisement.
Reject Any Clinic That:
- Offers "same day veneers in 1 hour", a true full Smile Design cannot be executed in an hour; even a compressed single-visit workflow takes 3–7 days
- Will not perform a physical mock-up before tooth preparation
- Cannot show you your proposed smile rendered digitally on your own facial photograph
- Has no in-house master ceramist, and cannot name the laboratory where your ceramic will be fabricated
- Does not take pre-treatment photographs from a standardised protocol
- Will not provide a diagnostic wax-up
- Uses a single generic shade (B1 for everyone) regardless of age, skin tone, or face shape
- Has no night-guard protocol for bruxers
- Refuses to explain the difference between feldspathic, lithium disilicate, and zirconia, or cannot recommend which is appropriate for your case
- Quotes a price without seeing your teeth, your bite, and your facial photographs
- Guarantees a specific outcome ("Hollywood smile in 3 days") before clinical assessment
- Pressures you to commit on the day of inquiry or offers a "today-only" discount
- Has no published or accessible warranty terms in writing
- Outsources everything with no in-house digital capacity
- Has no structured remote follow-up protocol for international patients
- Has no recourse pathway if something fails after you return home
- Has no independent reviews, no long-term case documentation, and no complications transparency
What a Safe Clinic Looks Like:
- DSD-driven or equivalent digital-design workflow
- Physical mock-up approval gate before preparation
- Named master ceramist on staff or on a named partner bench
- Three-specialist case review (prosthodontist + cosmetic lead + ceramist)
- Specialist-led care
- Internationally recognised ceramic systems (Ivoclar, GC, 3M, Dentsply)
- Hospital-grade sterilisation
- Published clinical outcomes and internal registry
- Written warranty document with replacement policy
- Night guard included for all patients, not "if you want one"
- Structured pre-op, intra-op, and post-op protocols
- Transparent itemised pricing
- A real, contactable post-op support system in Canada
- Willingness to tell you when their treatment is not the right fit for you
At Stunning Dentistry
We helped draft the framework above using the same criteria we would want a loved one to apply before choosing an aesthetic clinic in any country. We are equally comfortable being rejected on our own test. If after reading this you are not convinced we pass every checkpoint, walk away. The Canadian dental-tourism industry has grown partly because some operators hid behind glossy marketing. Our response is transparency over persuasion. We would rather you flew to a different clinic and had a great outcome than flew to us because you felt pressured.
Canadian Patient Stories, Real Journeys, Real Outcomes
The patient experiences referenced here are paraphrased from consented patient testimony. Names and locations have been generalised for privacy. Clinical outcomes are accurate.
Jessica, 32, Vancouver
Brendan, 47, Toronto
Priya, 38, Montreal
At her 72-hour mock-up appointment, she cried. She had not seen her own teeth without the grey shadow since she was a child. She approved the mock-up, the preparation was conservative, minimum-prep depths because her enamel was intact, and the final ceramic was delivered on Day 7. Total clinical fee: CAD 19,500. Total out-of-pocket including flights, hotel, and her partner as companion: CAD 23,800. At her 24-month review, no complications, shade stability confirmed by cross-polarised photography, no marginal staining, no gingival changes.
We do not publish patient stories as marketing, we publish them because Canadian readers asked us to. Every story above is consented, fact-checked against the clinical record, and edited only to protect privacy. We are happy to put new prospective patients in direct touch with previous Canadian patients (with their explicit permission) at the consultation stage.
At Stunning Dentistry
Jessica, Brendan, and Priya are not curated success stories. They are three of the more than three hundred Canadian Smile Design patients we have treated since the start of 2022. Their outcomes are typical, not exceptional, that is the point. We chose them because they reflect the three most common Canadian aesthetic journeys: the wedding-focused young patient, the mid-life bruxism-driven rehabilitation, and the long-standing discolouration case the local market had declared too difficult. Whichever profile you most resemble, we have walked alongside someone like you before. The path is mapped. We can put you in touch.
Partner Dentists in Canada, Our Network Roadmap
Honesty first: as of April 2026, our in-Canada partner network is in active expansion. We do not pretend to have a clinic on every corner. Here is exactly where we stand and where we are going.
What Is Live Today
- Remote follow-up: 24/7 CRM, structured Zoom protocol, prosthodontist-led photograph review, operational now for every Canadian patient.
- Canadian hygienist roster: vetted hygienists in Toronto, Vancouver, Montreal, Calgary, and Edmonton comfortable working around ceramic margins, with full clinical records sharing.
- Emergency referral pathway: confirmed referral relationships with select Canadian cosmetic dentists for urgent in-person assessment and debonded-veneer re-cementation under our warranty terms.
What Is Building Through 2026
- Formal partner-clinic agreements in Toronto, Vancouver, Montreal, and Calgary, clinics where in-person review, routine maintenance, and emergency re-bonding can happen as part of an integrated pathway
- Annual in-Canada clinical day visits by a Stunning Dentistry prosthodontist, on a rotating basis, for patient reviews and prospective consultations
- A published partner-clinic directory with credentials, scope of supported services, and patient feedback
What This Means for You
- Full-quality clinical care during your visit
- A structured remote follow-up that works
- A clear emergency pathway in Canada if something goes wrong
- A network roadmap that expands the in-person Canadian touchpoints throughout the year you are under our care
We will not oversell what does not yet exist. The remote follow-up is excellent. The in-person Canadian footprint is growing. Both will be true on the day you book and both will be better six months later.
At Stunning Dentistry
We made a deliberate decision not to fabricate an Canadian "presence" we do not yet hold. Plenty of dental-tourism operators list partner clinics that turn out to be a phone-forwarding number. We list only what is operational today and what is in active expansion this calendar year. When the formal partner-clinic agreements are signed in Toronto, Vancouver, Montreal, and Calgary, this section will be updated with the named clinics, the credentialled clinicians, and the specific scope each one supports. Until then, the remote model carries the load, and it carries it well. We would rather under-promise and outperform than the reverse.
Clinics Near You, Which Stunning Dentistry Location Fits Your Trip
Stunning Dentistry operates from India's largest dental hospital footprint, with multiple locations equipped for Smile Design. The right destination for your trip depends on your origin city in Canada, your flight preference, and your post-treatment recovery preference.
Our Aesthetic-Capable Locations for Smile Design Cases
What Is the Same Across Every Location
- Specialist-led prosthodontic and cosmetic team under Dr. Priyank Sethi's clinical oversight
- Identical intraoral scanning, DSD App, Exocad, CAD/CAM, and 3D printing infrastructure
- Same Ivoclar, GC, and 3M ceramic systems
- Same written warranty
- Same 24/7 CRM support pathway
- Same pre-op, intra-op, and post-op protocols
What Differs
- Volume of international aesthetic programmes (Hyderabad runs the largest international program by volume and has the deepest master-ceramist bench for complex hand-layered anterior cases)
- Adjacent travel/recovery options (city character, recovery hotel options, post-treatment tourism opportunities)
- Direct vs one-stop flight options from your origin Canadian city
How We Help You Choose
At Stunning Dentistry
One clinical governance framework, one SOP library, one warranty, one accountability chain. Whether you fly into Hyderabad, Delhi, Mumbai, or Bangalore, the DSD workflow is the same, the ceramic systems are the same, the prosthodontist-cosmetic-ceramist pairing is the same, and the post-treatment pathway is the same. Every clinician treating you has been trained on the same internal protocol and audited against the same outcomes registry. A patient is never "downgraded" by choosing the city closer to their layover or their extended family. The clinical experience is uniform across the footprint. That uniformity is a deliberate engineering choice, not an accident of scale.
| Location | Access from Canada | Best For |
|---|---|---|
| **Hyderabad, Flagship Hospital** | Direct/1-stop from Toronto, Vancouver, Montreal, Calgary via Singapore/KL | Most complex cases, full-mouth Smile Design, master-ceramist hand-layered feldspathic, full international patient infrastructure |
| **Delhi NCR** | Direct/1-stop from major Canadian capitals | Patients combining treatment with North India travel |
| **Mumbai** | 1-stop from major Canadian capitals | Patients combining treatment with Mumbai or West India travel |
| **Bangalore** | 1-stop from Toronto, Vancouver | Patients with family/connections in South India |
Clinical References
This article references peer-reviewed research from:
- Beier US, Kapferer I, Burtscher D, Dumfahrt H (2012), "Clinical performance of porcelain laminate veneers for up to 20 years." International Journal of Prosthodontics, the 20-year cohort dataset cited for 95.2% at 10 years and 82.9% at 20 years
- Gurel G, Sesma N, Calamita MA, Coachman C, Morimoto S (2013), "Influence of enamel preservation on failure rates of porcelain laminate veneers." International Journal of Periodontics & Restorative Dentistry, APR technique and minimum-preparation outcomes
- Magne P, Magne M, Belser U (2003), "The esthetic width in fixed prosthodontics." Journal of Prosthodontics, tooth proportion and golden proportion evidence base
- Coachman C, Calamita M (2012), "Digital Smile Design: A tool for treatment planning and communication in esthetic dentistry." Journal of Cosmetic Dentistry, DSD App methodology
- Friedman MJ (1998, 2005), "A 15-year review of porcelain veneer failure, a clinician's observations." Compendium of Continuing Education in Dentistry
- Layton DM, Walton TR (2012, 2017), systematic reviews of ceramic restoration survival, Journal of Prosthodontics and International Journal of Prosthodontics
- Christensen GJ (various), practical decision frameworks for composite vs porcelain veneer selection, Journal of the American Dental Association
- Chu SJ (2003), "Range and mean distribution frequency of individual tooth width of the maxillary anterior dentition." Practical Procedures and Aesthetic Dentistry, proportion references
- Frush JP, Fisher RD (1958), dentogenic theory and smile arc definition, Journal of Prosthetic Dentistry
- Lombardi RE (1973), "The principles of visual perception and their clinical application to denture esthetics." Journal of Prosthetic Dentistry, foundational aesthetic framework
- Kokich VO, Kiyak HA, Shapiro PA (1999), "Comparing the perception of dentists and lay people to altered dental esthetics." Journal of Esthetic Dentistry, midline and aesthetic-deviation thresholds
- Ward DH (2007), "A study of dentists' preferred maxillary anterior tooth width proportions: comparing the recurring esthetic dental proportion to other mathematical and naturally occurring proportions." Journal of Esthetic and Restorative Dentistry
- Gresnigt MM, Kalk W, Ozcan M (2013, 2019), clinical performance of direct and indirect composite veneers
- Wolff D, Kraus T, Schach R, Pritsch M, Mente J, Staehle HJ (2020), long-term outcomes of direct composite veneers
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
How is Smile Design different from just getting veneers?
Smile Design is the planning discipline; veneers are one of the restorations that may be used within it. You can have veneers without Smile Design, that is what happens when a clinic places veneers tooth-by-tooth without facial-integrated design, mock-up approval, or occlusal engineering. The outcomes are predictably worse. Smile Design wraps the veneers (and crowns, and gingival work where needed) in a structured planning workflow so the smile is designed as a system.
What materials do you use for veneers?
We use three primary ceramic systems: feldspathic porcelain (hand-layered by the master ceramist, most translucent, used for anterior aesthetic excellence in patients without high bite force), lithium disilicate / E.max (press-or-milled, higher strength, most commonly used across the modern Smile Design smile line), and monolithic zirconia (highest strength, used for full-coverage posterior crowns in high-bite-force patients). The material is chosen per tooth based on function and aesthetic demand, not a single-material default across the case.
Can I see the final result before committing?
Yes, this is the central tenet of the mock-up approval gate. A physical mock-up of the proposed smile is seated on your teeth on Day 2 of the workflow, and you wear it for 48–72 hours before any preparation is done. You photograph, speak, eat, and share the mock-up. You approve it in writing before we proceed. The final ceramic must match that mock-up in shape, proportion, and architecture.
What is the warranty on my Smile Design?
Stunning Dentistry provides a written warranty at delivery. The warranty covers: ceramic material defects, bonding failure not attributable to trauma or wilful neglect, and mechanical failure of the restoration in normal function. The warranty explicitly does not cover: trauma (sports injury, car accident), wilful neglect of night guard use, failure to attend documented annual reviews, and non-dental events. Full terms are in the written document you receive on the day of delivery.
How long does the whole process take?
Compressed visit at Stunning Dentistry: 8–10 days in India for a standard Smile Design without orthodontic pre-treatment. Staged approach: 6–9 months if Invisalign pre-treatment is indicated, plus 10 days for the Smile Design visit. Complex cases with gingival surgery or vertical dimension correction: 10–14 days compressed, or two visits spaced 6–8 weeks apart.
Will my gums change colour or shape after veneers?
Properly finished veneer margins produce no gingival colour change. Gingival response at 4–8 weeks post-cementation is typically full tissue health, with papillae at their final height. Where you may see change is if the veneers replaced older PFM crowns, the blue-tinted gingiva around PFM margins typically resolves within 3 months once the metal substructure is removed.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.