Full Mouth RehabilitationRebuilding Structure, Function, Occlusion, and Aesthetics Across Every Tooth
- Full mouth rehabilitation at Stunning Dentistry rebuilds or replaces every functional tooth surface across one or both arches, All-on-4, All-on-6, zygomatic implants, crown-and-veneer reconstruction, or combination cases.
Cost: CAD $10,000–$18,000 for a full-arch implant protocol, compared to CAD $50,000–$80,000 with Canadian prosthodontists.

Full-Arch Rehabilitation
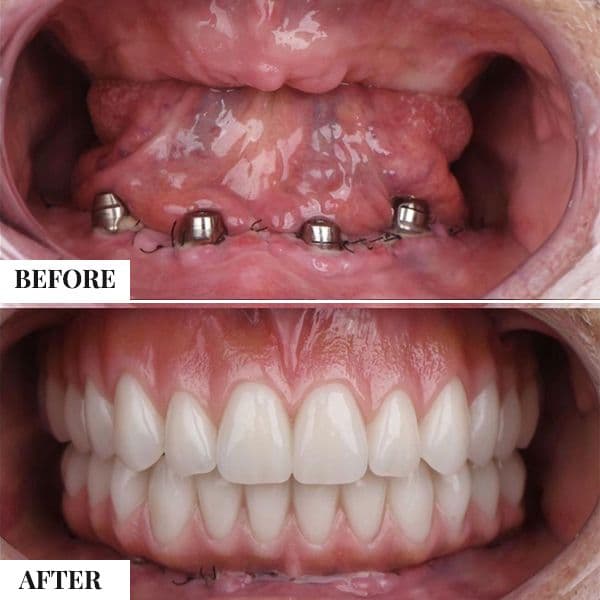
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Immediate Load
Full-arch or multiple implant cases where provisional teeth are placed shortly after surgery in suitable clinical conditions.

Multiple Implant Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.

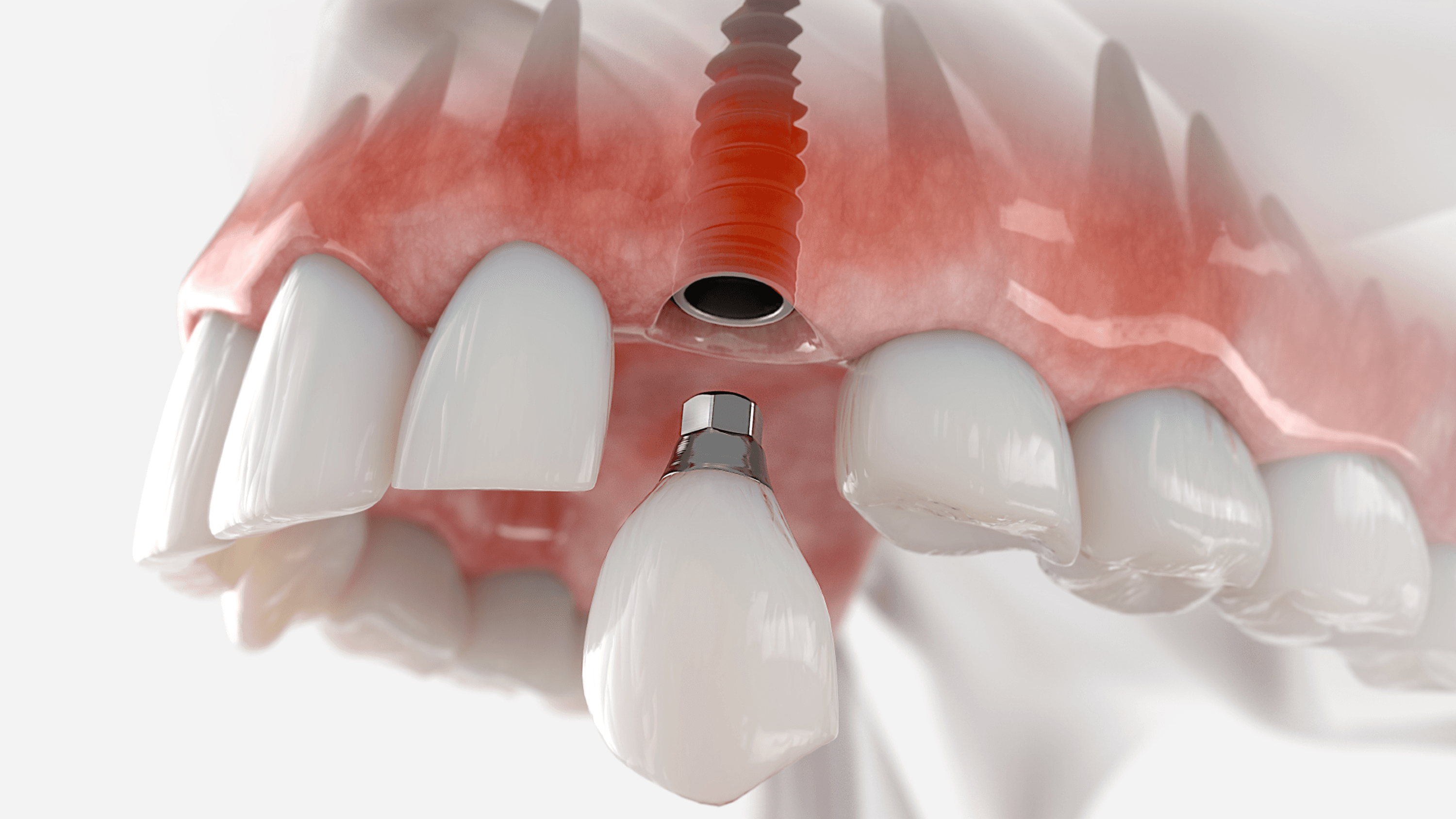
Single Tooth Implant
Single-tooth replacement with an implant and crown for a natural-looking, long-lasting result.

Bone Grafting & Advanced Surgical Support
Regenerative procedures performed to establish adequate bone volume for stable implant placement.

Revision & Complex Implant Cases
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Overview
Full Mouth Rehabilitation is the comprehensive restoration of every tooth, or every functional site where a tooth should be, across one or both dental arches. It is the category of dentistry that re-engineers four things at once: structure, function, occlusion, and aesthetics, all against the background of periodontal and systemic health.
Full Mouth Rehabilitation is not a shortcut. It is the most demanding category of restorative dentistry, built on nearly a century of peer-reviewed functional-occlusion research, Dawson, Kois, Pankey, Hobo and Takayama, and delivered today with digital tools those same clinicians would have considered science fiction.
For patients reading from Canada
The Full Mouth Rehabilitation pathway available here is the same rehabilitation category practised by prosthodontists in Toronto, Vancouver, Montreal, Calgary, and Edmonton. The diagnostic frameworks (Dawson, Kois, Pankey), the occlusal principles (centric relation, anterior guidance, canine-protected occlusion), the implant protocols (All-on-4, All-on-6, zygomatic), and the material standards (monolithic zirconia, lithium disilicate, PEKK) are internationally consistent. What changes when you travel to Stunning Dentistry is not the clinical protocol, it is the specialist bench depth, the in-house digital infrastructure, and the total cost. We walk through exactly how that comparison lines up further down this page.
At Stunning Dentistry
Every Full Mouth Rehabilitation case carries a dual-clinician sign-off: Dr. Priyank Sethi and one senior prosthodontist review and countersign the plan before any irreversible treatment begins. That dual-signature protocol is the single most important safeguard in comprehensive dentistry, because once you cross the line from a ten-unit case into a full-arch reconstruction, there is no solo-clinician shortcut that ages well. The protocol is named SD-FMR-05 and it runs on every case in every location we operate.
What Full Mouth Rehabilitation Actually Means
Full Mouth Rehabilitation, abbreviated here as FMR, is the simultaneous or sequentially staged restoration of:
- Every remaining tooth that can be preserved, restored to functional form and load-bearing ability
- Every missing tooth site replaced by an implant, bridge unit, or removable prosthesis component
- The occlusal scheme that governs how the upper and lower arches meet, glide, and protect one another
- The vertical dimension of occlusion (VDO) that determines facial height, lip support, and jaw muscle balance
- The periodontal foundation that has to carry whatever we build on top of it
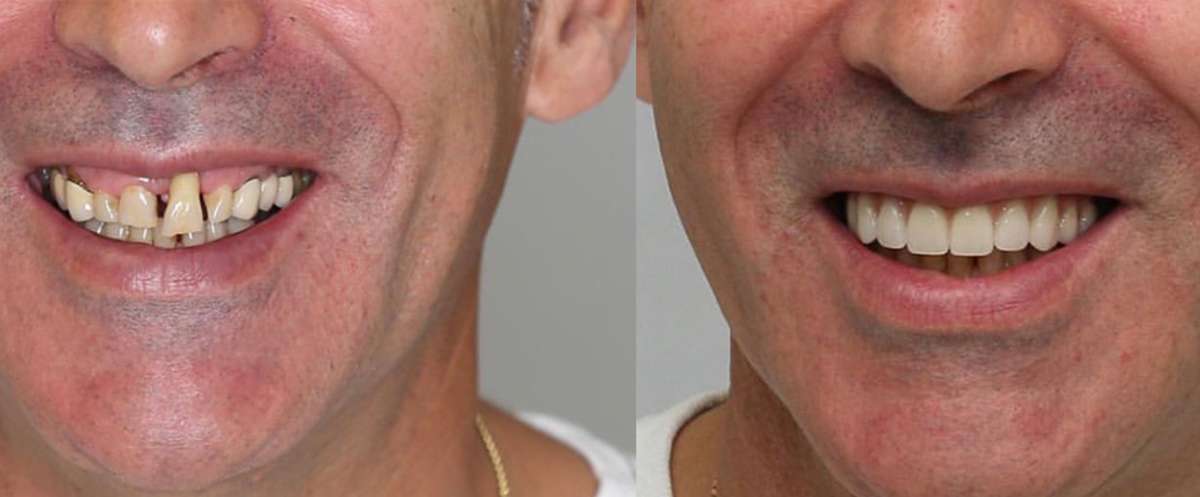
- The aesthetic outcome, smile line, incisal display, buccal corridor, lip dynamics
A patient with twelve failing crowns across both arches, severe attrition, a collapsed bite, and worn anterior guidance is a Full Mouth Rehabilitation case. A patient with two broken molars is not, even though the treatment uses the same materials.
What Full Mouth Rehabilitation Is Not
- It is not "a lot of crowns." It is a redesigned bite.
- It is not cosmetic dentistry, though aesthetics are part of the outcome.
- It is not a single-specialist exercise. It is team dentistry.
- It is not a one-trip, one-surgery event. It is a staged sequence over months.
At Stunning Dentistry
The moment a consultation starts crossing from "restorative treatment plan" into "full mouth rehabilitation", the case is pulled out of the single-clinician workflow and into our SD-FMR-05 protocol. That means a full diagnostic workup, a dual-clinician plan review, a three-stage patient approval gate, and sequencing that protects reversibility until the very last phase. The line between complex restorative dentistry and full mouth rehabilitation is one of the most commonly crossed without declaration, and one of the most important to declare.
When Full Mouth Rehabilitation Is Indicated
Full Mouth Rehabilitation is indicated when the dentition has deteriorated, or never developed, to a point where individual-tooth treatment cannot restore function and form. The clinical scenarios that drive FMR fall into seven categories.
1. Severe Tooth Wear
- Attritional, mechanical tooth-on-tooth wear, often driven by bruxism or parafunction
- Erosive, chemical dissolution by dietary acids, gastric reflux, or occupational exposure
- Abrasive, mechanical wear from external agents such as toothbrush abrasion or hard-object chewing
- Abfractive, cervical stress lesions that compound other wear patterns
2. End-Stage Periodontal Disease
3. Failed Large Restorations
4. Congenital Conditions
- Amelogenesis imperfecta, defective enamel formation, clinically varying from hypoplastic to hypomineralised forms
- Dentinogenesis imperfecta, defective dentine, often associated with osteogenesis imperfecta
- Ectodermal dysplasia, multiple missing teeth with associated soft-tissue, hair, and sweat-gland abnormalities
- Severe hypodontia or oligodontia, congenital absence of six or more permanent teeth excluding third molars
5. Traumatic Destruction
6. Failed Prior Rehabilitation
7. Psychogenic Bruxism Complications
Severe, sustained bruxism in psychogenic form, driven by stress, sleep-disordered breathing, or psychiatric comorbidity, can destroy a dentition in five to ten years. When a full-arch of teeth shows flat, polished wear facets across all cusps, cracked cusps on multiple molars, and anterior incisal edges worn to gingival level, an FMR combined with a long-term splint regime and behavioural therapy is often the only durable solution.
At Stunning Dentistry
The seven indications above drive roughly 85 per cent of all our Full Mouth Rehabilitation caseload. The remaining 15 per cent are mixed presentations, congenital overlap with trauma, periodontal overlap with bruxism, failed prior work overlap with new erosive disease. We have seen every permutation, which is why SD-FMR-05 starts with a category assignment rather than a treatment proposal. You cannot plan the rebuild until you have named the thing you are rebuilding from.

The Diagnostic Frameworks That Guide Every Case
Full Mouth Rehabilitation without a named diagnostic framework is carpentry, not dentistry. Four frameworks, each with decades of peer-reviewed literature and international clinical teaching, structure every FMR case at Stunning Dentistry.
The Dawson Concept
The Kois Technique
The Pankey Philosophy
The Hobo and Takayama Twin-Stage Technique
Our complex reconstruction cases, bruxism-driven rehabilitations and post-orthodontic restorations, routinely use twin-stage sequencing.
At Stunning Dentistry
The four frameworks above are not used interchangeably. Each case is assigned a lead framework during diagnostic review based on the predominant clinical problem: Dawson for collapsed bites with suspected CR-MIP discrepancy, Kois for aesthetic-led rehabilitations, Pankey for behaviourally complex patients who benefit from extended provisional testing, and Hobo twin-stage for high-bruxism or post-orthodontic precision cases. The framework assignment is the first page of every SD-FMR-05 case file. It is the instruction manual for the build.
Core Occlusal Concepts You Need to Understand
Full Mouth Rehabilitation is, at its core, occlusal engineering. A reader without the vocabulary will struggle to have a meaningful consultation. Here is the glossary your prosthodontist will use, explained plainly.
Vertical Dimension of Occlusion (VDO)
Centric Relation (CR) vs Maximum Intercuspation (MIP)
The Posselt Envelope of Motion
Canine-Protected vs Group Function Occlusion
- Canine-protected occlusion, the canines are the only contacting teeth in lateral excursion; posterior teeth disclude. Preferred for most reconstructions because the canine is the longest-rooted tooth and is anatomically designed to bear lateral loads.
- Group function, multiple posterior teeth contact in lateral excursion. Tolerable in intact natural dentitions but harder to reproduce reliably in reconstructed cases.
Anterior Guidance
- Shallow guidance, small overjet/overbite, flat guidance angle, tolerates wide envelope of function but transmits less disclusion to posterior teeth
- Steep guidance, large overjet/overbite, steep angle, strong posterior disclusion but narrower envelope; intolerant of bruxism unless splinted
The Envelope of Parafunction
The Christensen Phenomenon
Described by Carl Christensen in 1905, the Christensen phenomenon is the posterior separation that occurs when the mandible protrudes, because both condyles slide down the articular eminences, creating a wedge-shaped gap at the posterior teeth. If a reconstruction ignores the Christensen phenomenon, posterior contacts in protrusion can interfere, overload, and fracture. Twin-stage Hobo reconstruction is specifically designed to manage this.
At Stunning Dentistry
The eight concepts above are not vocabulary we test patients on. They are the vocabulary we write the treatment plan in. Every FMR report we issue references the measured CR-MIP slide, the VDO at rest and occluded, the freeway space, the planned guidance scheme, and the Christensen-phenomenon compensation built into the posterior cusp angles. The patient receives a plain-English summary; the dentist-to-dentist report carries the full terminology. Both are true. Both are on file.

The Five Modalities of Full Mouth Rehabilitation
When Full Mouth Rehabilitation is indicated, the real clinical decision is which modality, or combination of modalities, fits the case. There are five modalities and several common combinations. Each has genuine indications, and each has honest limitations.
- Fixed upper plus overdenture lower, the pragmatic compromise when maxillary bone allows fixed work and mandibular cost or medical risk favours a removable option
- Orthodontic preparation plus restorative, alignment first, then restoration, for cases where malpositioned teeth make a direct restorative approach impossible
The next sections summarise the three full-arch implant modalities as teasers, with full depth on their dedicated pages.
All-on-4 Full Arch Fixed
All-on-4 is the foundational full-arch implant protocol, four implants per arch, tilted posteriors, immediate provisional, fixed prosthesis. Developed by Dr Paulo Malo in the 1990s, published in its first major clinical study in 1998, commercially launched by Nobel Biocare in 2004, and now treating more than 250,000 patients worldwide.
- The entire rehabilitation (both arches All-on-4)
- The upper arch (combined with a lower tooth-supported rehabilitation)
- The lower arch (combined with an upper zygomatic or tooth-supported case)
Read the full protocol: All-on-4 Dental Implants, Fixed Teeth on Four Implants
At Stunning Dentistry
All-on-4 is one tool in the FMR kit, not the default answer. When the bone, bite, and patient profile all point to it, it is an excellent choice. When the case is aesthetic-led, or the bone allows for more implants, or the patient presents with extreme maxillary atrophy, we redirect to All-on-6, zygomatic, or a tooth-supported build. The FMR decision is never made inside a single procedure, it is made by comparing across all five modalities. The All-on-4 page reads cleanly because the protocol is clean; the decision to use it is the part we take seriously.
All-on-6 When Bone Allows
All-on-6 adds two implants to the All-on-4 configuration, producing a six-implant full-arch fixed prosthesis. The extra implants shorten cantilevers, distribute load across more supporting sites, and provide redundancy if a single implant fails.
- Bone volume genuinely supports six implants without grafting
- The patient has a high bite force or confirmed bruxism profile
- The arch is long (wide anteroposterior dimension)
- The patient or clinician values the redundancy of an extra supporting site
Read the full protocol: All-on-6 Dental Implants, Six-Implant Full Arch
At Stunning Dentistry
The All-on-4 vs All-on-6 decision is one of the most common FMR decisions we make. Our internal default is All-on-4 when the biomechanics check out, All-on-6 when the bone, bite, or arch geometry makes the extra implants clinically meaningful. The choice is recorded in the SD-FMR-05 case file with the reasoning, not "patient preferred more implants" but the specific CBCT finding, bite-force reading, or AP-spread calculation that drove the call. Six implants in the wrong position are not better than four implants in the right position.
Zygomatic When Bone Is Gone
Zygomatic implants bypass the maxilla entirely. Instead of engaging residual alveolar bone, they anchor into the zygomatic bone, the cheekbone, through an extended implant body of 30–55 mm. Developed by Professor Per-Ingvar Brånemark in 1988 and refined through the Nobel Biocare zygomatic platform, the protocol is reserved for severe maxillary atrophy where conventional implants are not placeable even with grafting.
Read the full protocol: Zygomatic Implants, When Conventional Bone Is Gone
At Stunning Dentistry
We have treated zygomatic cases for Canadian patients who were told in three separate consultations in Toronto, Vancouver, and Calgary that fixed teeth were "impossible" without eighteen months of iliac-crest grafting. The remote CBCT review at the start of those journeys revealed zygomatic candidacy that their original consultations had not explored. We mention this not to cast shade but because a real proportion of Canadian "no you can't" quotes are not zygomatic-literate, and the patient deserves to know the full menu before accepting the worst option on it.
Teeth-in-a-Day: Immediate Loading
Teeth-in-a-Day is not a separate modality, it is a loading strategy applied across the full-arch implant protocols. The principle: when primary implant stability at placement exceeds the defined threshold (typically 35 Ncm insertion torque or equivalent ISQ value), a provisional fixed prosthesis can be fitted on the same day as surgery. The patient leaves with fixed, functional teeth.
Read the full protocol: Teeth-in-a-Day, Immediate-Load Full-Arch Implants
At Stunning Dentistry
Teeth-in-a-Day is an offer we earn on the day of surgery, not one we promise at consultation. " A proportion of FMR cases, somewhere around one in eight, do not meet the torque threshold at placement and are loaded conservatively. The outcomes for those cases are equally good; they just look different on day one. Overpromising same-day teeth to every patient is one of the most common misrepresentations in full-arch implant marketing. We do not play that game.
Smile Design for Aesthetic-Led Cases
Smile Design, Digital Smile Design (DSD) in its current computer-assisted form, is the aesthetic planning layer over every Full Mouth Rehabilitation that involves visible teeth. Developed by Dr Christian Coachman (Brazil) from the mid-2000s onward, DSD integrates facial photography, video analysis, intraoral scan data, and digital wax-up into a single planning environment.
- What should the incisal display look like when the patient speaks?
- What is the ideal upper lip line in smile?
- Where should the midline sit relative to the philtrum and the facial midline?
- What tooth proportions fit this face, width-to-height ratio, golden proportion, or golden percentage?
- What is the buccal corridor contribution to the smile width?
Read the full protocol: Smile Design, Digital Aesthetic Planning
At Stunning Dentistry
Every FMR case with any anterior tooth involvement runs through Digital Smile Design before the prosthodontic plan is signed off. The mock-up is the patient's veto moment, if the mock-up does not match their expectation, we redesign. Once the mock-up is approved, it becomes the template for every subsequent restoration. This is not aesthetic theatre; it is a reversibility gate. The irreversible preparation starts only after the patient has seen, tried, and signed off on the outcome.
Full Mouth Tooth-Supported Rehabilitation
Not every FMR is implant-based. When the remaining dentition is substantially intact, structurally, periodontally, and endodontically, but compromised by severe wear, drifting, or extensive failing restorations, the right answer is often full-mouth tooth-supported rehabilitation: 28 to 32 restorations (crowns, onlays, veneers) across the natural dentition.
- Remaining teeth have good periodontal prognosis (pocket depths <4 mm, no mobility beyond grade I, radiographic bone loss <30 per cent)
- Endodontic prognosis is favourable or pre-existing root canal treatments are adequate
- Ferrule is sufficient on compromised teeth (a minimum 1.5–2 mm of sound tooth structure above the finish line)
- Patient's age and systemic profile favour tooth preservation over surgery
- The wear or damage pattern is addressable by restoration without extraction
The lifespan of a well-executed tooth-supported FMR is 15–25 years for the ceramic restorations, 10–20 years for composite-supported components. Periodic replacement or refurbishment is part of the long-term plan.
At Stunning Dentistry
Tooth-supported FMR is the modality many patients underestimate and many clinicians under-recommend. It is preservation-focused, avoids surgery, uses the patient's own roots, and produces beautiful aesthetic outcomes when executed with the Kois 6-step diagnostic and a proper provisional testing phase. It is also demanding, sequencing, periodontal work, and ceramist-level execution. max and zirconia restorations to Zirkonzahn PlanOral articulator settings derived from the patient's own condylar recordings.
Hybrid Implant Plus Tooth Restoration: and Why We Avoid It
A hybrid restoration splints a natural tooth and an implant together in one prosthesis, a crown, a bridge, or a multi-unit framework. It appears to be the pragmatic middle ground: keep the natural tooth, add the implant, join them under one restoration.
When a case appears to require it, for example, a long-span span where both natural teeth and implants are available for support, we design the prosthesis in segments, with the tooth-supported segment separate from the implant-supported segment, and no rigid connection between them. This preserves the independent movement of the tooth and the ankylosed integrity of the implant.
At Stunning Dentistry
The hybrid-splinting decision is where we have declined cases that a Canadian referring dentist had proposed in good faith. The refusal is not a criticism of the referrer; it is a reflection of an evidence base (Naert 2001, Lang 2004, Pjetursson 2007) that has strengthened over twenty years. We document our rationale in the treatment plan, we propose the segmented alternative, and we explain it to the patient in plain English. The hybrid model exists in the clinical world; it does not exist in ours.
Implant Overdentures and Combination Cases
When fixed full-arch implant work is either not clinically indicated or not financially accessible, implant overdentures, removable prostheses retained by 2–4 implants per arch, are an excellent intermediate modality.
- Bar-retained, a milled bar connects the implants, and the overdenture clips onto the bar. Maximum retention, maximum distribution of load, highest cost.
- Locator attachments, individual abutments on each implant with a nylon insert in the denture. Moderate retention, simple to service, middle cost.
- Ball attachments, spherical abutments with a metal housing in the denture. Lowest cost, highest wear, most frequent maintenance.
The Upper Fixed, Lower Overdenture Combination
This combination is not a compromise in the pejorative sense; it is a pragmatic, well-documented configuration with its own published evidence base. For many patients, it is the best total outcome per dollar invested.
At Stunning Dentistry
The upper fixed, lower overdenture combination is a modality we proactively propose when the case profile favours it. We do not treat it as the fallback option. It is a deliberate clinical configuration that many patients, once they understand the trade-offs, actively prefer over dual-arch fixed work. The consultation includes hands-on time with both options, a provisional fixed prosthesis to feel, and a demonstration overdenture on the bar system, so the choice is made with tactile knowledge, not verbal description.
The Interdisciplinary Team: Who Does What
Full Mouth Rehabilitation is not single-clinician dentistry. The protocol requires a coordinated team, and the quality of the FMR outcome is bounded by the weakest member of the team. Here is who does what.
Prosthodontist
Periodontist
Endodontist
Oral Surgeon
Implantologist
Orthodontist
- Intrusion of supra-erupted teeth to recover VDO
- Extrusion to gain ferrule for compromised teeth
- Rotation correction for cosmetic alignment
- Space redistribution to create restorable gap geometry
- Temporary anchorage devices (TADs) for complex movements
TMJ and Pain Specialist
Laboratory Technician
- Digital articulator mounting
- CAD design of provisionals and definitives
- Milling, sintering, staining, and glazing of ceramic restorations
- Verification of passive fit
- Shade communication and final characterisation
At Stunning Dentistry, the lab is in-house and works on the same campus as the clinical team. No courier delays, no lost impressions, no "we'll see it when the box arrives".
At Stunning Dentistry
The seven-specialty interdisciplinary team above sits under one clinical governance framework and meets weekly for complex FMR case rounds. The meeting is not a formality; it is a case-by-case review where each specialty sees the full picture before any phase is committed. A periodontist who sees only the gums and an orthodontist who sees only the teeth produce a fragmented plan. A team that sees the whole mouth, the whole face, and the whole patient produces coherent dentistry. The SD-FMR-05 protocol mandates the team round-table on every case above a defined complexity threshold.
The Digital Workflow: 2025–2026 Standard
Full Mouth Rehabilitation in 2026 is a digital discipline. The analogue steps that remain, manual occlusal adjustment, human ceramist characterisation, hand articulation checks, are the ones that still matter. Everything else has gone digital.
Intraoral Scanning
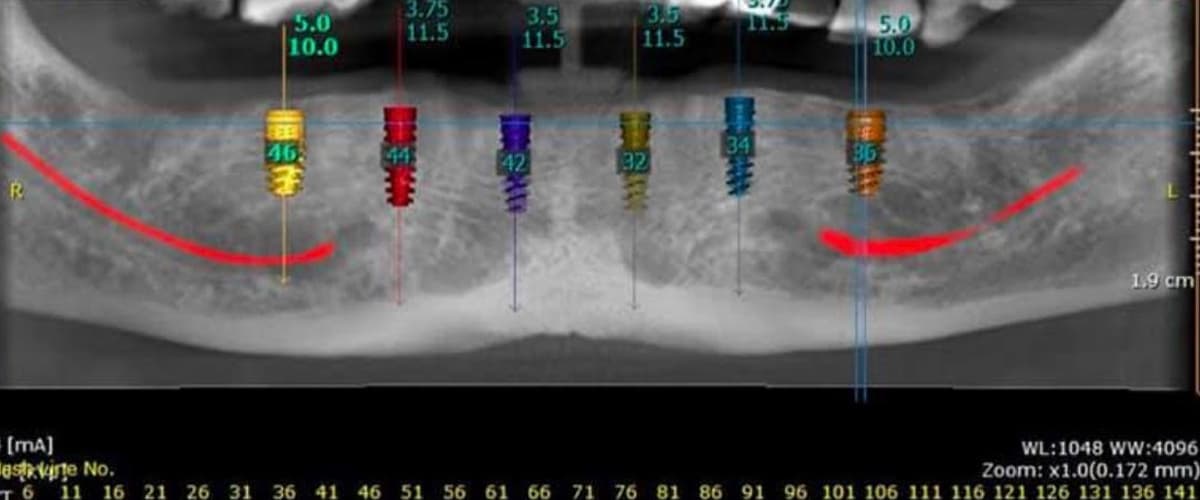
Cone Beam CT
Digital Smile Design
Virtual Articulator
- Zirkonzahn PlanOral, the virtual articulator in the Zirkonzahn Modellier CAD environment, with condylar inclination and Bennett angle settings configurable to the patient's own ARCUSdigma-recorded values
- Ceramill Articulator, the Amann Girrbach equivalent, used on cases exported to our Ceramill-based milling lines
- Kois Model Articulator, used for Kois-sequenced cases where the Kois Analyser provides the reference planes
The Mock-Up Fabrication and Approval Gate
- An additively printed PMMA try-in
- A subtractively milled PMMA shell cemented over the unprepped or minimally prepped teeth
- A direct composite mock-up transferred from a silicone index
The Three-Stage Patient Approval Gate
Provisional to Definitive
Definitives are milled from the approved provisional file, with material changes (PMMA to zirconia, PMMA to lithium disilicate, PMMA to layered e.max) but with geometry preservation. What works in the provisional is what gets delivered in the definitive.
At Stunning Dentistry
The digital workflow above is identical to the workflow used in the best specialist prosthodontic practices in Canada, North America, and Europe. The difference is that ours runs end-to-end in one building: scanner to CBCT to design suite to mill to sintering oven to try-in chair, all within one clinical governance framework. No courier turnaround to an external lab, no version-control drift between practice and lab software, no shade miscommunication between a clinician and a ceramist who have never met. One building, one team, one workflow. That is what makes the protocol reproducible at volume.
Materials Used for the Definitive Rehabilitation
Material selection in FMR is clinical, not cosmetic. Each material has a bite-force ceiling, an aesthetic ceiling, a wear behaviour, and a retrievability profile.
Monolithic Zirconia
- 3Y-TZP (3 mol% yttria), highest flexural strength at 1,100–1,200 MPa, lower translucency, best for posterior load-bearing
- 4Y-TZP, middle ground at 900–1,000 MPa, improved translucency
- 5Y-TZP, 800–900 MPa, most translucent, best for anterior aesthetics
- Multilayer zirconia (Prettau-style, Katana Multi-Layered), gradient from 3Y body to 5Y incisal, balancing strength and aesthetics
Lithium Disilicate
- IPS e.max Press and CAD, flexural strength 360–400 MPa, excellent translucency, outstanding shade integration
- Vita Suprinity (zirconia-reinforced lithium silicate), flexural strength 420 MPa, similar aesthetic profile with slight strength gain
CAD-CAM PMMA
Porcelain-Fused-to-Metal (PFM)
PEKK and Pekkton
Polyetherketoneketone, a high-performance thermoplastic with flexural strength around 200 MPa but remarkable impact resistance and fatigue performance. Used at Stunning Dentistry for:
- Implant bar substructures under overdentures
- Hybrid prosthesis frameworks where weight and shock absorption matter
- Bruxism-prone cases where a degree of shock dissipation is clinically desirable
At Stunning Dentistry
Material selection for every FMR case is recorded position-by-position in the treatment plan. max with bonded porcelain, lower canines and posteriors monolithic zirconia". The material logic is documented, the decision rationale is on file, and the patient's own preferences, for translucency, metal avoidance, or specific brand, are reconciled against the clinical indications before the plan is locked.
The Evidence Base for Full Mouth Rehabilitation
Full Mouth Rehabilitation is one of the most intensively studied categories of dentistry. The evidence base that anchors our protocol:
- Pjetursson et al. 2014, a systematic review of multi-unit fixed restoration survival, published in the *Journal of Clinical Periodontology*, documenting 10-year survival of 89.1 per cent for implant-supported fixed partial dentures and 90.7 per cent for tooth-supported FPDs
- Abduo 2011, review of rehabilitation outcomes in severe tooth wear, *Journal of Oral Rehabilitation*, establishing the evidence base for increased VDO in wear cases
- Ahlers 2008, bruxism management protocols, *Schmerz* (German pain journal), establishing splint-therapy standards
- Sheldon 2000, outcomes of Pankey-philosophy rehabilitations, *Journal of Prosthetic Dentistry*
- Dawson 2007, *Functional Occlusion: From TMJ to Smile Design*, Mosby/Elsevier, the definitive textbook on functional occlusion
- Naert et al. 2001, tooth-to-implant connected prosthesis outcomes, *International Journal of Prosthodontics*, the foundational evidence against hybrid splinting
- ITI Consensus Reports, International Team for Implantology consensus reports on mixed fixed-removable restorations, ongoing publication cycle
- Malo et al. 2019, 18-year prosthetic survival for All-on-4, *Journal of Dental Research* supplementary data
- Kois Center Publications, ongoing publication of the Kois Technique through the Kois Center and peer-reviewed prosthodontic journals
- Hobo and Takayama 1997, *Twin-Stage Procedure in Restorative Dentistry*, Quintessence
- Bartlett, Ganss, and Lussi 2008, BEWE scoring system for erosive wear, *Clinical Oral Investigations*
- Tucker and colleagues 2018, erosion typology, *British Dental Journal*
At Stunning Dentistry
The twelve-citation reference list above is the headline. The working reference library that informs SD-FMR-05 runs to more than three hundred peer-reviewed publications, catalogued and indexed in our clinical governance portal. Every clinician treating an FMR case can pull up the specific publication that supports the specific decision at any moment. Evidence-based dentistry is a phrase that gets used loosely; we treat it as an operational requirement, not a marketing claim.
Candidacy: Medical, Dental, Psychological
FMR candidacy is evaluated across three domains. All three have to pass before treatment is confirmed.
Medical Candidacy
- Bleeding disorders, von Willebrand disease, haemophilia, platelet dysfunction. Requires haematology consultation and perioperative management plan.
- Anticoagulation therapy, warfarin, DOACs (apixaban, rivaroxaban, dabigatran), antiplatelet therapy (aspirin, clopidogrel). Requires coordinated bridging or continuation protocol with the prescribing physician.
- Immunosuppression, organ transplant medications, chemotherapy, biological therapy for autoimmune disease. Implant outcomes are still acceptable in many cases but require case-by-case medical clearance.
- Uncontrolled diabetes, HbA1c above 8 per cent is a relative contraindication. Target HbA1c for elective implant surgery is below 8 per cent, ideally below 7 per cent.
- Bisphosphonate and anti-resorptive therapy, oral bisphosphonates (alendronate, risedronate) with extended use, IV bisphosphonates (zoledronic acid, pamidronate), and denosumab. Medication-related osteonecrosis of the jaw (MRONJ) risk requires specific protocols per AAOMS position paper.
- Active malignancy or radiation to the head and neck, significant modifier of surgical risk and implant survival.
Dental Candidacy
- Parafunction control, bruxism must be manageable, ideally with a splint history demonstrating compliance. Uncontrollable bruxism without a management plan is a contraindication for most FMR modalities until resolved.
- Active caries, must be controlled before definitive work. Holding restorations are placed in the provisional phase.
- Active periodontal disease, pocket depths, bleeding, suppuration all have to be resolved in a pre-restorative periodontal phase.
- Endodontic status, retained root fragments, necrotic pulps in strategic teeth, all addressed before restorative work begins.
- Oral hygiene capacity, realistic assessment of the patient's ability to maintain a full-mouth restoration. If hygiene is the limiting factor, an overdenture or a simpler modality may be preferred.
Psychological Candidacy
Often overlooked. The psychological screen covers:
- Realistic expectations, the patient understands that FMR is a rebuild, not a rejuvenation miracle, and that maintenance is lifelong
- Capacity for multi-visit commitment, an FMR is 14–30 months in specialist Canadian practice and 8–14 months at Stunning Dentistry under consolidated travel scheduling
- Body dysmorphic disorder screening, patients presenting with extreme aesthetic preoccupation benefit from pre-treatment psychological review
- Parafunction origin assessment, psychogenic bruxism responds to FMR only when the behavioural driver is addressed alongside
At Stunning Dentistry
Candidacy is decided by a three-specialist review: the lead prosthodontist, an independent prosthodontist on the clinical board, and the relevant subspecialty (implantologist for fixed full-arch cases, periodontist for perio-led cases). The review is documented, dated, and signed. If any of the three flags a concern, the case is paused and the concern resolved before treatment is confirmed. We have declined FMR cases at the candidacy gate, patients whose bite could have been restored but whose periodontal compliance, bruxism control, or systemic medical picture made the predicted long-term outcome unacceptable. That filter protects both the patient and the treating team.
Full Mouth Rehabilitation Modalities Compared
The headline comparison across the five modalities, on the variables patients most commonly ask about.
At Stunning Dentistry
The comparison table above is printed and handed to every FMR consultation patient before a single treatment proposal is made. Reading it in full changes the conversation from "how much does this cost" to "which modality is the best fit for me and why". The table exists because a transparent modality comparison is the most protective document in dentistry: it shows what is on offer, what it delivers, and what it costs, side by side. Clinics that steer patients to one modality without showing the full ladder are underserving those patients. We publish the ladder.
| Variable | Full-arch Fixed Implant (All-on-4 / All-on-6) | Full-arch Tooth-Supported Rehabilitation | Hybrid Implant + Tooth | Implant Overdenture | Conventional Complete Denture |
|---|---|---|---|---|---|
| **Lifespan of prosthesis** | 15–20+ years (zirconia definitive) | 15–25 years (e.max/zirconia) | Variable, lower due to biomechanical mismatch | 7–12 years on nylon/locator components; bar 15+ years | 5–7 years |
| **Lifespan of foundation** | 20–30+ years (implant bone-integration) | Dependent on periodontal health of abutment teeth | Compromised, tooth intrusion risk | 20–30+ years (implants) | N/A, ridge resorbs over time |
| **Total cost (Stunning Dentistry, CAD, full mouth)** | $21,000–$40,000 All-on-4 / All-on-6 dual arch | $11,000–$22,000 (28 units) | Not offered | $9,000–$16,000 dual arch 2–4 implants | $2,800–$5,200 dual arch |
| **Total cost (AU specialist, full mouth)** | $55,000–$95,000 | $42,000–$90,000 | Variable, not recommended | $18,000–$35,000 | $4,500–$9,000 |
| **Maintenance intensity** | Moderate, annual review, screw checks, hygienist every 3–6 months | High, multiple natural teeth to maintain | Variable | Moderate-high, nylon replacements every 6–18 months | Low clinical, high daily |
| **Aesthetic ceiling** | Very high with zirconia and flange design | Highest, uses natural tooth emergence | Variable | High but removable flange compromises some cases | Moderate, removable constraint |
| **Bite force recovery (% natural)** | 80–95% | 85–100% | 60–80% | 60–80% | 10–20% |
| **Primary candidacy** | Edentulous or terminal dentition, bone available or zygomatic rescue | Intact dentition with wear, drift, or failing restorations | Not offered | Edentulous, cost-conscious, tissue-acceptance | Edentulous, medically unfit for surgery or budget-constrained |
| **Number of trips at Stunning Dentistry (AU patient)** | 2 trips across 6–8 months | 2–3 trips across 8–12 months | N/A | 2 trips across 4–6 months | 1–2 trips across 2–4 months |
| **Total treatment time** | 4–8 months including healing | 8–14 months including perio/ortho prep | Variable | 4–6 months | 2–4 months |
The FMR Journey by Case Complexity: Three Tiers
Not every FMR runs on the same timeline. The clinical complexity dictates the sequence, the trip count, and the total duration. We categorise FMR journeys into three tiers.
Tier 1: Consolidated FMR (8–10 Months, 2 Trips)
- Single-arch or dual-arch full-arch fixed implant work (All-on-4 or All-on-6)
- No major grafting required
- No pre-restorative orthodontics
- No complex periodontal surgery
- Stable systemic health
- Trip 1 (10–14 days): diagnostics, surgical planning, extractions, implant placement, immediate provisional
- Home period (4–6 months): osseointegration, remote follow-up
- Trip 2 (7–10 days): definitive prosthesis try-in and delivery, final occlusal balancing
Tier 2: Staged FMR (12–16 Months, 3 Trips)
- Tooth-supported full-mouth rehabilitation with pre-restorative periodontal work
- FMR combining implants with significant tooth-supported components
- Moderate bone grafting required before implant placement
- Pre-restorative orthodontics (6–10 months)
- Bruxism management requiring documented splint-therapy phase
- Trip 1 (10–14 days): diagnostics, periodontal surgery if needed, orthodontic start, splint fitting
- Home period (4–8 months): orthodontic treatment, splint wear, periodontal healing
- Trip 2 (10–14 days): implant placement and/or tooth preparation, provisional FMR delivered
- Home period (3–6 months): provisional testing phase, VDO adaptation
- Trip 3 (7–10 days): definitive prosthesis try-in, delivery, final balancing
Tier 3: Complex FMR (14–18 Months, 3–4 Trips)
- Zygomatic implant cases
- Severe atrophy cases requiring staged grafting before implant placement
- Full mouth rehabilitation in congenital conditions (amelogenesis, ectodermal dysplasia)
- Revision FMR after failed prior rehabilitation
- Orthognathic surgical component
- Trip 1 (10–14 days): diagnostics, preliminary surgery (extractions, grafting, or orthognathic prep)
- Home period (4–6 months): graft integration, orthognathic healing, provisional denture phase
- Trip 2 (10–14 days): definitive implant placement (including zygomatic if indicated), immediate or delayed loading
- Home period (4–6 months): osseointegration, provisional FMR wear
- Trip 3 (10–14 days): definitive prosthesis fabrication, try-in, delivery
- Trip 4 (optional, 5–7 days): final refinement, aesthetic adjustment, long-term review initiation
Total time from consultation to completion: 14–18 months.
At Stunning Dentistry
The tier assignment is made at the end of the first consultation, based on the Kois 6-step diagnostic outcome. We share the tier with the patient transparently, along with the rationale and the projected trip schedule. Tier inflation, calling a tier 1 case a tier 2 or 3 to justify more trips, is a documented pattern in some international dental tourism. Our direction of drift is the opposite: we consolidate trips where the clinical pathway allows. An efficient, shorter journey with equivalent outcomes is what we are trying to build, not a longer one.
What Determines the Cost of Full Mouth Rehabilitation
Cost Variables
- Number of implants, zero, two, four, six, eight, or zygomatic implant inclusion, each tier adding cost
- Number of ceramic units fabricated, from a 12-unit partial rehabilitation to a 28–32 unit full-mouth rebuild
- Material selection, PMMA provisional is lowest cost, IPS e.max mid-tier, monolithic zirconia higher, layered zirconia highest
- Periodontal surgery requirement, scaling-and-root-planing-only is relatively low cost; regenerative grafting and crown lengthening add substantially
- Orthodontic preparation, short-duration aligner therapy is moderate cost; full fixed orthodontics with TADs is higher
- Endodontic retreatment, each retreated tooth adds cost
- Bone grafting, ridge preservation is low; lateral augmentation mid; sinus lift higher; iliac crest grafting highest
- Zygomatic inclusion, zygomatic implants carry a cost premium over conventional implants reflecting hospital-grade infrastructure and extended surgical time
- Single-arch vs dual-arch scope, one arch treatment is roughly 55–65 per cent of dual-arch cost (fixed costs of diagnostics, articulation, and team setup do not double)
- Revision-case complexity, removing prior failed work and re-planning adds time and cost
What the Investment Reflects
- Specialist team time across prosthodontics, periodontics, endodontics, oral surgery, orthodontics
- CBCT imaging and digital planning
- Intraoral scanning and digital smile design
- Virtual articulator-driven design
- Hospital-grade sterile surgical environment for implant and surgical phases
- In-house CAD-CAM and 3D printing laboratory
- Provisional testing phase in PMMA before definitive commitment
- Definitive prosthesis fabrication in the selected material
- Warranty coverage, lifetime on implants, defined coverage on prosthetic components
- Long-term maintenance infrastructure, annual reviews, radiographs, CRM continuity
Canadian Specialist Quotes vs Stunning Dentistry Pricing
We publish the comparison transparently. These are CAD ranges current as of April 2026, reviewed quarterly.
What the Canadian specialist quote typically reflects: private prosthodontic and surgical specialist fees, Canadian laboratory costs, Canadian compliance and overhead, premium implant systems. Provincial health plans do not cover FMR. Employer supplemental dental plans contribute CAD 2,500–3,000 per calendar year at most for dental rehabilitation, with lifetime orthodontic cover in the CAD 10,000–25,000 band on some policies. Marginal against an CAD 55,000 figure.
Cost figures current as of April 2026, reviewed quarterly. Your CRM manager will confirm the live position at booking.
At Stunning Dentistry
The CAD ranges above are not promotional prices; they are the operating ranges across the full spread of FMR complexity we see. A straightforward dual-arch All-on-4 in a healthy patient lands near the lower end. A complex zygomatic-plus-All-on-4 case with significant pre-surgical work lands near the upper end. We do not move figures in response to how eager a patient seems or how far they have flown. The band is the band, the variables are the variables, and the specific number is determined by the specific case, not the specific patient's negotiating skill.
| FMR Modality (full mouth, dual arch unless noted) | Canada (private specialist quote, CAD) | Stunning Dentistry (CAD equivalent) | Indicative Saving |
|---|---|---|---|
| Full-arch fixed All-on-4 (both arches, zirconia) | 55,000–95,000 | 21,000–32,000 | 55–65% |
| Full-arch fixed All-on-6 (both arches, zirconia) | 65,000–110,000 | 26,000–40,000 | 55–65% |
| Full-arch zygomatic (extreme atrophy, upper + lower rehabilitation) | 75,000–130,000 | 28,000–48,000 | 55–65% |
| Full-mouth tooth-supported (28 IPS e.max / zirconia units) | 42,000–90,000 | 11,000–22,000 | 65–75% |
| Staged orthodontic + restorative full mouth rehabilitation | 30,000–70,000 | 14,000–28,000 | 55–65% |
| Upper All-on-4 fixed + Lower 4-implant overdenture | 40,000–65,000 | 15,000–25,000 | 60–70% |
| Upper zygomatic full-arch + Lower All-on-4 | 60,000–100,000 | 24,000–38,000 | 55–65% |
The Interdisciplinary Team Role Matrix
A quick-reference matrix showing which specialist leads which phase of an FMR case. The prosthodontist is the coordinating lead on every case.
At Stunning Dentistry
Every FMR case carries a named specialist for each active role on the matrix. You know who is placing your implants. You know who is designing your occlusion. You know who is fabricating your prosthesis. You know who is managing your bruxism splint. There are no anonymous "the team will handle it" handoffs. Accountability is personal, documented, and, in the case file, signed for. The SD-FMR-05 protocol requires individual clinician sign-off at each phase transition. Nothing moves forward without a named signature.
| Phase | Prosthodontist | Periodontist | Endodontist | Oral Surgeon / Implantologist | Orthodontist | TMJ / Pain | Lab Technician |
|---|---|---|---|---|---|---|---|
| Initial consultation and diagnosis | Lead | Supporting | Supporting | Supporting | Supporting | Supporting | , |
| Kois 6-step analysis | Lead | Consulting | Consulting | Consulting | Consulting | Consulting | , |
| Periodontal stabilisation | Coordinating | Lead | , | , | , | , | , |
| Endodontic management | Coordinating | , | Lead | , | , | , | , |
| Crown lengthening | Coordinating | Lead | , | , | , | , | , |
| Pre-restorative orthodontics | Coordinating | , | , | , | Lead | , | , |
| Extractions and bone grafting | Coordinating | Supporting | , | Lead | , | , | , |
| Implant planning (digital) | Co-lead | , | , | Co-lead | , | , | Supporting |
| Implant placement (All-on-4/6) | Supporting | , | , | Lead | , | , | , |
| Zygomatic implant surgery | Supporting | , | , | Lead (specialist) | , | , | , |
| VDO determination | Lead | , | , | , | , | Supporting | Supporting |
| Digital Smile Design | Lead | , | , | , | , | , | Co-lead |
| Virtual articulator setup | Lead | , | , | , | , | Consulting | Lead |
| Provisional fabrication | Lead | , | , | , | , | , | Lead |
| Splint therapy | Supporting | , | , | , | , | Lead | Supporting |
| Definitive prosthesis fabrication | Lead | , | , | , | , | , | Lead |
| Definitive delivery and occlusal balancing | Lead | , | , | , | , | Supporting | Supporting |
| Long-term maintenance (annual review) | Lead | Supporting | , | Supporting | , | Supporting | Supporting |
Step-by-Step: How Full Mouth Rehabilitation Runs at Stunning Dentistry
Phase 1: Remote Pre-Screening (Before You Fly)
Upload existing panoramic X-ray, CBCT, or intraoral photographs via the patient portal. Submit written medical and dental history. 30–45 minute Zoom consultation with a senior prosthodontist. Preliminary tier assignment (Tier 1, 2, or 3) and trip-count estimate. If international travel is confirmed, diagnostic imaging plan and booking schedule issued.
Phase 2: In-Clinic Diagnostic Workup (Day 1–3 of Trip 1)
CBCT volumetric imaging (full-head and TMJ capture), full-mouth intraoral scan (Trios 5 or Primescan), facial and intraoral photography, video capture of speech and smile dynamics, full periodontal charting, endodontic pulp testing on strategic teeth, Kois 6-step diagnostic assessment, Dawson bimanual manipulation and CR verification, VDO measurement (rest and occluded), and CR-MIP slide measurement.
Phase 3: Team Treatment Planning (Day 3–4 of Trip 1)
Lead prosthodontist assembles the diagnostic data. Multi-specialty team round-table (prosthodontist + periodontist + implantologist + endodontist + orthodontist as relevant). Digital Smile Design preview. Virtual articulator setup using recorded condylar data. Written FMR treatment plan delivered to patient. Dual-clinician sign-off under SD-FMR-05. Three-stage patient approval gate initiated.
Phase 4: Plan Approval Gate (Day 4–5 of Trip 1)
Patient reviews the written plan with the lead prosthodontist, questions answered, modifications considered, plan signed off, costs confirmed in writing, and schedule for all subsequent phases issued.
Phase 5: Pre-Restorative Work (Remainder of Trip 1 and Home Period)
Depending on case tier: extractions of hopeless teeth, implant placement (All-on-4, All-on-6, or zygomatic), periodontal surgery (pocket reduction, crown lengthening, regenerative procedures), endodontic treatment or retreatment, orthodontic appliances (for tier 2 and 3 cases), and splint fitting for bruxism cases.
Phase 6: Mock-Up Approval Gate (Early Trip 2)
Intraoral mock-up fitted (additive PMMA shell or silicone-index transfer), reviewed by the patient in photos, mirror, conversation, and with family. Modifications requested or mock-up signed off.
Phase 7: Provisional FMR Delivery and Testing (Trip 2)
Full-mouth PMMA provisional prosthesis delivered. Functional test drive in real-world conditions for 3–6 months at home. Weekly to monthly remote follow-up. Modifications made remotely where possible, or at a mid-cycle visit if needed.
Phase 8: Provisional Approval Gate (Start of Trip 3)
Patient reviews the provisional performance, remaining modifications identified, provisional signed off as the geometric template for definitive fabrication.
Phase 9: Definitive Fabrication (During Trip 3)
Approved provisional scanned into CAD environment. Definitive prosthesis milled from zirconia, IPS e.max, or PFM per the plan. Ceramist characterisation (staining, glazing, layering). Try-in appointment with aesthetic and functional verification.
Phase 10: Definitive Delivery and Occlusal Balancing (End of Trip 3)
Definitive FMR delivered. Occlusion balanced under T-Scan or articulating paper in digital articulator settings. Hygiene reinforcement, night guard fitted, warranty documentation issued, long-term maintenance schedule activated.
Phase 11: Long-Term Maintenance (Lifetime)
Annual Zoom review, radiographic monitoring, screw torque verification for implant cases, and night guard replacement, detailed in the Aftercare section below. Warranty coverage remains active for the life of the restoration.
At Stunning Dentistry
The eleven-phase protocol above is written, versioned as SD-FMR-05, and internally audited on every case. Every prosthodontist, every surgeon, and every lab technician works from the same SOP. Your FMR on a Tuesday in Hyderabad runs on the same protocol as an FMR on a Thursday in Delhi. That is what single-practice clinical governance looks like, and it is what lets us stand behind the warranty.
Aftercare and Long-Term Maintenance
A Full Mouth Rehabilitation is the starting line of a maintenance partnership, not the finish line of a construction project. Long-term outcomes in FMR are a collaboration between the clinical team and the patient.
Daily at Home
- Brush twice daily with a soft-bristled or electric toothbrush. Technique matters more than duration. For screw-retained implant prostheses, focus on the interface between the prosthesis and the soft tissue.
- Water floss the full mouth once daily. For full-arch implant work, angle the tip at 45 degrees into the prosthesis-gum interface. For tooth-supported work, the water flosser complements, not replaces, interdental brushes.
- Superfloss or interdental brushes, for implant-supported prostheses, superfloss (braided tufted floss) is the single most effective daily hygiene aid. For tooth-supported FMR, interdental brushes (TePe or similar) matched to the embrasure size.
- Wear your night guard every night if one has been fitted. Non-negotiable for bruxism-history patients.
- Avoid extreme loads, ice, bones, prying packaging open, hard candy.
- Report early, new mobility, persistent bleeding, metallic taste, prosthesis movement, or pain. Small problems caught early stay small.
Every 3–6 Months
- Professional hygiene visit. We coordinate with a Canadian hygienist for in-person maintenance between your Stunning Dentistry visits. The visit includes sub-prosthetic cleaning, gingival health assessment, plaque index measurement, and hygiene technique reinforcement.
Annually
Every 5–10 Years
Without Maintenance
Published data on mechanical complication rates in FMR run 25–40 per cent over long-term follow-up, chipping, screw loosening, peri-implantitis, periodontal progression on supporting teeth. Structured maintenance materially reduces these rates. The patients whose FMR looks excellent at year 15 are not lucky. They are the patients who kept every annual review.
At Stunning Dentistry
Long-term maintenance is built into the original treatment plan, not tacked on at delivery. Your year-one reviews, your radiograph schedule, your night-guard fittings, your hygienist visits are scheduled before you leave India and tracked in our clinical portal. For Canadian patients, we coordinate the in-person visits with your local hygienist or dentist partner where one is in our network, and run the specialist reviews remotely with the same prosthodontist who led your case. The clinical relationship does not end at the airport.
Myths vs Clinical Reality
Myth
** Full Mouth Rehabilitation is just "a lot of crowns".
Reality
** FMR is a redesigned bite. The number of restorations is an output, not the defining feature. The defining features are the re-engineered VDO, the redesigned occlusal scheme, the planned anterior guidance, and the staged multi-specialty sequencing.
Myth
** You can do a full mouth in one week.
Reality
** An FMR completed in one week is almost certainly missing the provisional testing phase, which means the patient is receiving a definitive restoration without verification. Our tier 1 FMR is 8–10 months total. Shorter is not better; shorter is undertested.
Myth
** If my teeth are still there, I do not need to worry about VDO.
Reality
** VDO loss is progressive with wear. Patients with severe attrition typically present with 4–6 mm of lost vertical dimension, collapsed anterior guidance, and a sunken lower-face profile. Rebuilding VDO is central to the wear-case FMR.
Myth
** Zirconia is always better than IPS e.max.
Reality
** Material choice is position-specific. Zirconia is better for posterior load-bearing in high-bite-force patients. IPS e.max is better for anterior aesthetics and bonded indirect work on adequately preserved tooth structure. A good FMR uses both.
Myth
** If implants fail, the whole case fails.
Reality
** In modern FMR, implant failure is usually recoverable. For All-on-4, a single failed implant can often be replaced or the prosthesis converted to a three-implant support temporarily. For tooth-supported FMR, a failing tooth can be extracted and replaced with an implant in the next cycle without rebuilding the entire arch.
Myth
** If I go overseas for FMR, I cannot get it maintained in Canada.
Reality
** Maintenance is modular. Hygiene, radiographs, photographs, and routine checks can be done by any Canadian dentist. Complex issues can be referred back, handled remotely, or managed via our Canadian emergency referral pathway. The pathway is documented, not improvised.
Myth
** Every FMR needs implants.
Reality
** Tooth-supported FMR is a valid and often preferable modality when the native dentition is periodontally and structurally sound. Implant-first thinking is a common bias; preservation-first thinking is frequently the right clinical answer.
Myth
** Bruxers cannot have FMR.
Reality
** Bruxers can have FMR, but the case design changes. Material selection favours monolithic zirconia. Cusps are flatter. Anterior guidance is shallower. A splint regime is mandatory. And the patient's bruxism is ideally managed medically or behaviourally alongside.
At Stunning Dentistry
Myths above are not strawmen. They are the specific misconceptions we encounter most often at consultation, catalogued across fifteen years of full-mouth practice. We rebut them not to persuade but to educate. A patient who understands why a claim is true or false can make a better decision. Our job is not to protect our clinical preferences from patient questioning, it is to equip patients to question, and to make their decision on evidence.
People Also Ask
Short, direct answers to the questions search engines consistently surface for Full Mouth Rehabilitation. Depth follows in the FAQ.
Severe wear, multiple failing restorations, collapsed bite, chronic periodontal disease with multiple compromised teeth, congenital conditions, traumatic damage. A comprehensive diagnostic assessment confirms whether an FMR approach is indicated.
At Stunning Dentistry
The ten People Also Ask items above reflect the actual search-engine surface for Full Mouth Rehabilitation. Our answers are the same answers we give on the phone, at consultation, in email, and in writing. Consistency between a curious reader's experience and a signed-up patient's experience is the simplest integrity test a dental clinic can take.
Ask Your Doctor: 12 Questions for Your Consultation
Whether you consult with us or with any clinic offering full mouth rehabilitation, these are the questions a good doctor will welcome. If any are deflected, you have learned something important.
1. Is my case fixed-implant or tooth-supported, or some combination? Show me the reasoning.
Acceptable answers walk you through the bone, the periodontal status, the structural state of remaining teeth, and the relative pros and cons of each modality. Evasive answers or immediate recommendations without comparative reasoning are a flag.
2. How many visits will this require, and over what time frame?
Honest tier assignment. A tier 1 case in 8–10 months. A tier 2 case in 12–16 months. A tier 3 case in 14–18 months. Claims of one-week or one-month full mouth rehabilitation are almost always skipping the provisional testing phase.
3. What lab materials will you use, tooth by tooth?
You should see a treatment plan that specifies monolithic zirconia at positions x, y, z; IPS e.max at a, b, c; PFM or alternative where clinically indicated. A plan that says "ceramic" or "zirconia" across the whole arch without position-specific rationale is less considered.
4. What will my splint be, and when will I start wearing it?
Michigan hard acrylic for canine-protected cases, Tanner or similar for specific indications. Splint fitting timing, during provisional, at definitive delivery, or before any restoration in bruxism-diagnostic mode, should be specified.
5. What about my TMJ symptoms? How will they be managed?
A clinician comfortable with FMR-TMJ intersection will describe diagnostic splint therapy, CR verification, condylar imaging if indicated, and how the planned occlusion interacts with the joint. An evasive answer here is concerning.
6. What is your refurbishment and remake policy, in writing?
Ask for the written warranty document. Read it. Ask specifically what is covered, what is excluded, for how long, and what the claim process looks like.
7. What happens if a tooth fails mid-treatment?
The plan should include contingency for unexpected endodontic failure, periodontal deterioration, or structural breakdown of a strategic tooth during treatment. Ask what happens and what it costs.
8. Will you show me the CBCT and the digital plan before any irreversible work?
Yes is the only correct answer. You should see your own bone, the planned implant positions (if any), the DSD mock-up, and the written treatment plan before any preparation starts.
9. Who specifically is performing each phase of my case?
Named prosthodontist, named surgeon, named orthodontist, named periodontist. If the answer is "the team" without names, ask again.
10. Will there be a provisional testing phase?
Yes, there should be. A full-mouth PMMA provisional worn for 3–6 months allows the VDO, the guidance, and the aesthetics to be verified in real-world conditions before definitive fabrication. Skipping this phase is a major red flag.
11. What is the maintenance protocol for the next 10 years, and what will it cost?
Annual reviews, radiographs, hygiene visits, splint replacements, possible minor refurbishments. Ask for a 10-year projected maintenance schedule.
12. What is your contingency if I have a problem in 5 years and cannot easily reach your clinic?
For international patients this is critical. Our answer: 24/7 CRM manager, same-day Zoom triage, Canadian emergency referral pathway, flight-supported return for revision under warranty. Ask for their specific answer, in writing.
*Print this section. Take it to your consultation. A clinic that cannot answer these twelve questions clearly and in writing is not the right clinic, regardless of price.*
At Stunning Dentistry
We wrote this list knowing a proportion of readers will use it to choose a clinic other than us. We are comfortable with that. Our measure of success is not a higher booking rate; it is whether our Canadian patients arrive at the right clinical decision, with us or not. We answer every question above in writing for every FMR patient we treat. Ask for ours; we will send them.
Full Mouth Rehabilitation at Stunning Dentistry
Clinical Infrastructure
- 20 dedicated surgical and prosthodontic operatories within India's largest dental hospital
- In-house CAD-CAM and 3D printing laboratory, complete digital workflow from CBCT scan to final prosthesis, with no external lab dependency
- Hospital-grade sterilisation: over 90 per cent single-use materials, HEPA air purification, multi-layer sterilisation protocols
- Zirkonzahn, Amann Girrbach, and Dentsply Sirona digital design and milling platforms
- Trios 5 and Primescan 2 intraoral scanners
- GE Healthcare and Planmeca CBCT imaging platforms
Clinical Governance
Every FMR case is treatment-planned under Dr Priyank Sethi's oversight (MDS Prosthodontics, Ph.D. in Dentistry, 15+ years clinical experience) with dual-clinician sign-off. A named lead prosthodontist stays with the case through planning, provisional, and definitive phases. SD-FMR-05 protocol version-controlled and internally audited. Accredited with AAID, AACD, AAO, and BACD. Ranked No. 1 Dental Clinic in India for four consecutive years by Forbes India.
The Commitment
At Stunning Dentistry
The infrastructure listed above is not a marketing inventory; it is the operational backbone of a single-specialty dental hospital that performs more Full Mouth Rehabilitation cases in a quarter than most Canadian metropolitan specialist practices perform in a year. The CBCT, the milling unit, the sintering oven, the digital articulator, the sterilisation suite, all in the same building, under the same governance, under one signature of accountability. That is the precondition for the outcomes we publish. The building serves the patient. The team serves the protocol. The protocol is written down and it is signed for.
For Canadian Patients: Your Journey to India
We have built a structured, multi-trip pathway for Canadian FMR patients, not an improvisation. Unlike single-procedure dental tourism (All-on-4 alone, veneers alone), FMR is a multi-trip reality. Tier 1 cases need two trips. Tier 2 cases need three. Tier 3 cases need three or four. The journey below is the operating standard.
The Multi-Trip Model: Why It Is Not a Single Visit
- Osseointegration of implants takes 3–6 months, you cannot place implants on Monday and load them definitively on Friday
- Provisional testing in FMR takes 3–6 months, PMMA provisionals are designed to be lived with before definitive commitment
- Periodontal and endodontic stabilisation takes weeks to months
- Pre-restorative orthodontics (when needed) takes 4–10 months
- Bone grafting (when needed) takes 3–6 months to integrate
Typical Multi-Trip Schedules
- Trip 1 (10–14 days in India): full diagnostic workup, all surgery (implant placement, extractions), immediate provisional, aftercare
- Home period (4–6 months): osseointegration, remote follow-up, monthly Zoom reviews
- Trip 2 (7–10 days in India): definitive prosthesis design, try-in, delivery, final balancing, warranty activation
- Trip 1 (10–14 days): diagnostics, periodontal surgery or orthodontic initiation, preliminary work
- Home period (4–8 months): orthodontic treatment, periodontal healing, splint therapy, remote monitoring
- Trip 2 (10–14 days): implant placement and/or tooth preparation, full-mouth provisional delivered
- Home period (3–6 months): provisional testing phase, VDO adaptation, remote follow-up
- Trip 3 (7–10 days): definitive fabrication, try-in, delivery, final balancing
- Trip 1 (10–14 days): diagnostics, initial surgery (extractions, grafting, orthognathic prep if indicated)
- Home period (4–6 months): graft integration, orthognathic healing, provisional denture phase
- Trip 2 (10–14 days): definitive implant placement (including zygomatic if indicated), immediate or delayed loading
- Home period (4–6 months): osseointegration, provisional FMR wear, adaptation
- Trip 3 (10–14 days): definitive prosthesis design, try-in, delivery
- Trip 4 (optional, 5–7 days): final aesthetic refinement and long-term review initiation
What We Coordinate For You
Companion Travel
Companion travel is part of the protocol, not an extra. For the surgical trip (trip 1 in tier 1, trip 1 and trip 2 in tier 2, trips 1–2 in tier 3), a trusted companion, partner, family member, or friend, is strongly recommended. Recovery is straightforward, but having one person with you in-country improves safety, reduces post-op stress, and provides a backup communication channel if needed. Companion accommodation is shared-room; companion airport transfers are included.
At Stunning Dentistry
The multi-trip FMR journey is mapped trip by trip, day by day, before you leave Toronto, Vancouver, Montreal, Calgary, or Edmonton. You receive a printed itinerary for each trip, a clinical pathway diagram showing which phase each trip sits within, and a named CRM manager's WhatsApp number that persists across all trips. Nothing about the India visits is left to "we'll figure it out when you land next time". Dental tourism for FMR fails most often at the handoffs between trips, home-country maintenance, trip booking, schedule alignment with clinical readiness. We have engineered every handoff out of improvisation. Multi-trip continuity is the hard part, and it is the part we engineer the hardest around.
What This Costs in CAD: Your Out-of-Pocket Reality
Here is the full out-of-pocket figure for a Canadian FMR patient, not just the clinical fee. We publish this so the comparison with quoting in Toronto or Vancouver is honest, complete, and verifiable.
Tier 1 Dual-Arch All-on-4 FMR: Total CAD Cost (2 trips)
Tier 2 Staged FMR (Orthodontic + Restorative Full Mouth): Total CAD Cost (3 trips)
Tier 3 Complex FMR (Zygomatic + All-on-4): Total CAD Cost (3–4 trips)
Tier 1 Tooth-Supported Full-Mouth Rehabilitation (28 Units e.max/Zirconia): Total CAD Cost (2–3 trips)
What Insurance and Provincial Health Plans Cover
- Provincial health plans: Does not cover Full Mouth Rehabilitation. No exception.
- Employer supplemental dental plans (Canadian private cover): Typically reimburses CAD 2,500–3,000 per calendar year for dental treatment, depending on policy and waiting periods. Lifetime orthodontic cover ranges CAD 10,000–25,000 on some higher-tier policies.
- At Stunning Dentistry: Detailed itemised invoices issued for every line of treatment, suitable for private health claim submission upon return to Canada. Many of our Canadian patients recover CAD 3,000–6,000 across their FMR treatment window from their extras.
Cost figures current as of April 2026 and reviewed quarterly. Your CRM manager confirms the live position at consultation.
At Stunning Dentistry
The CAD out-of-pocket total above is the only number that should drive the decision against a Canadian quote. We do not quote clinical fees in isolation because that is how dental-tourism comparisons go wrong. Your Toronto out-of-pocket is flight-free; your India out-of-pocket is not. The honest comparison is total-to-total. We publish ours so you can run yours. If after flights, hotel, visa, insurance, and companion costs the net saving is under CAD 15,000 for an FMR case, we tell you at consultation. Flying is only worth it when the clinical depth, the specialist bench, and the arithmetic all point the same way.
| Line Item | CAD Range |
|---|---|
| Clinical fee at Stunning Dentistry (28 units ceramic, all-inclusive) | 11,000–22,000 |
| Return flights x 2–3 trips | 2,800–7,200 |
| Hotel accommodation (22–38 nights) | 2,200–6,500 |
| Visa, insurance, transport | 500–1,200 |
| Companion travel (optional) | 1,200–3,400 |
| **Total Canadian out-of-pocket** | **CAD 17,700–40,300** |
| Equivalent quote in Canada | **CAD 42,000–90,000** |
| **Net saving** | **CAD 24,000–50,000** |
Is This Worth Flying For? The Decision Framework
Travelling internationally for a Full Mouth Rehabilitation is a significant decision. FMR is more complex than single-procedure dental work, more trips, more months under treatment, more dependency on continuity. Here is the framework we ask Canadian patients to apply honestly.
When India Is Clearly the Right Call
- Your Canadian quote is CAD 45,000+ for the FMR and your net saving after travel exceeds CAD 15,000
- You are medically fit for international travel (not on active anticoagulation, not within 6 months of a cardiac event, no uncontrolled diabetes)
- You can commit to the trip schedule appropriate to your tier (2–4 trips across 8–18 months)
- You are comfortable with a structured remote-care model between trips
- You want access to in-house CBCT, CAD-CAM, 3D printing, virtual articulation, and a prosthodontist-led specialist team, without Toronto CBD pricing
- Your case complexity benefits from a higher-volume specialist bench
When India Is Not the Right Call
- Modest-scope rehabilitation where Canadian price differential is narrow
- Active health issues contraindicating international travel
- Inability to commit to remote follow-up between trips
- An established Canadian specialist relationship you value and do not want to interrupt
- Net savings, after honest accounting, below CAD 10,000 for FMR work
When to Get a Second Opinion First
- A clinic (in Canada or India) is pressuring you to commit on the day of consultation
- You have not seen your own CBCT, the materials plan, the written warranty, or the tier assignment
- You have been quoted an FMR for a suspiciously low price (under CAD 15,000 for dual-arch fixed implant work in India usually means budget implant systems without 10-year data, verify)
At Stunning Dentistry
We run between 30 and 50 free remote FMR consultations every month for Canadian patients, and a material proportion of them are advised to stay home. We earn no fee from those calls. We earn the trust of the patients we do treat, and the referrals their friends send the following year. Decisions made under sales pressure age badly. Decisions made with a clear-eyed framework tend to age well. We would rather lose a booking than win it the wrong way.
Pre-Travel Checklist for Canadian Patients
A practical, phase-by-phase list. Your CRM manager personalises it per case. This is the master.
10 Weeks Before Trip 1
- [ ] Submit CBCT or panoramic X-ray for remote pre-screening
- [ ] Complete medical history form
- [ ] Confirm fitness-to-travel with your Canadian GP, written clearance preferred
- [ ] Apply for India e-medical visa (5 working days processing)
- [ ] Book flights, confirm return no earlier than day 10 of trip 1
- [ ] Notify your private health insurer of planned overseas treatment
6 Weeks Before Trip 1
- [ ] Confirm hotel booking through our partner network
- [ ] Arrange travel insurance with international medical coverage and treatment-interruption protection
- [ ] Commit to the booking schedule deposit
- [ ] Confirm companion travel arrangements
- [ ] Refill regular prescriptions for the trip duration
- [ ] Book the GP visit closest to departure for final clearance
2 Weeks Before Trip 1
- [ ] Confirm airport pickup with CRM manager
- [ ] Pack soft foods and protein supplements for first 5 days post-surgery
- [ ] Charge and pack existing night guard if you have one
- [ ] Print your treatment plan, warranty summary, and emergency contact card
- [ ] Notify your bank of international travel
- [ ] Confirm SIM/eSIM for India
Day Before Departure
- [ ] Light meals if reflux is a concern
- [ ] Pack medications in carry-on, not checked luggage
- [ ] Confirm pickup time, hotel address, CRM manager phone in your phone
Between Trips
- [ ] Daily hygiene photo upload during first month post-op
- [ ] Monthly Zoom review attendance
- [ ] Book trip 2 flights based on CRM-confirmed clinical readiness date
- [ ] Maintain local hygienist visits per schedule
- [ ] Night guard wear compliance
Before Trip 2 and Subsequent Trips
- [ ] Confirm readiness via Zoom review 4 weeks before trip
- [ ] Re-book flights, hotel, transport per same partner network
- [ ] Confirm companion travel if applicable
- [ ] Review treatment progress and any modifications with CRM manager
At Stunning Dentistry
The multi-phase checklist above is not a generic dental-tourism template. It is our checklist, refined across more than 1,200 FMR and full-arch consultations, every item earned by a patient who once arrived unprepared. Each tick protects something specific: visa timing, insurance coverage, blood pressure on surgery day, SIM card working when your companion needs to call the clinic. Your CRM manager walks you through this, week by week, so nothing is left to "I think I have that covered".
Your Time in India: Multi-Trip Schedule
A real schedule for a real FMR journey. This example is a Tier 2 staged case, three trips, 14 months total, Upper All-on-4 + Lower tooth-supported 14-unit rehabilitation.
Trip 1: Diagnostics, Surgery, Initial Provisional (12 days)
Between Trip 1 and Trip 2: At Home in Canada (5 months)
- Week 1: hygiene photo upload, Zoom day 7 post-op review
- Week 2: Zoom review, upper arch stability check
- Month 1: Zoom consultation, intraoral photos reviewed by prosthodontist
- Month 2: Lower arch orthodontic progress review (Zoom)
- Month 3: Local hygienist visit (we provide referral)
- Month 4: Zoom review, preparation readiness assessment
- Month 5: Trip 2 confirmed, clinical readiness verified
Trip 2: Lower Arch Preparation and Full-Mouth Provisional (12 days)
Between Trip 2 and Trip 3: At Home in Canada (3 months)
- Weekly Zoom reviews during month 1
- Bi-weekly Zoom reviews during month 2
- Monthly review during month 3
- Local hygienist visit at month 2
- Full-mouth provisional testing throughout, VDO adaptation, speech refinement, aesthetic feedback, any modifications logged for trip 3 definitive
Trip 3: Lower Definitive Prosthesis and Final Delivery (8 days)
At Stunning Dentistry
The schedule above is the one we run, not the one we market. Surgery is on day 5 of trip 1 deliberately, not day 2, so your body has three days to settle before a major procedure and five days after to be watched closely before boarding a plane. Rest days are engineered, not accidental. Our FMR patients do not fly home with a bruised jaw and a vague follow-up instruction. They fly home with a printed discharge plan, reviews completed at days 1, 3, and 5 post-op, and the same prosthodontist on their phone.
| Day | What Happens |
|---|---|
| Day 1 | Arrival, hotel, rest |
| Day 2 | Final impressions and scans for lower definitive; occlusal records, aesthetic verification |
| Day 3 | Free day while lower definitive fabricated in-house |
| Day 4 | Lower definitive try-in; bite balance; aesthetic approval |
| Day 5 | Final delivery of lower definitive; full-mouth occlusal balancing; T-Scan or articulating paper verification |
| Day 6 | Night guard fitting; hygiene reinforcement; warranty activation |
| Day 7 | Final review, long-term maintenance schedule, discharge |
| Day 8 | Departure |
Back in Canada: Your Follow-Up Plan
The work is not finished when you board the final return flight. Long-term FMR success is built in the months and years that follow. Here is exactly how we maintain clinical oversight from across the ocean.
Year 1: The High-Vigilance Year
Years 2 Onwards
- Annual remote review by Zoom, clinical photos, hygiene photos, radiograph upload
- Annual in-Canada hygienist visit (we maintain a roster of Canadian hygienists comfortable supporting our FMR patients)
- Optional in-person review at Stunning Dentistry every 2–3 years if you would like a comprehensive clinical examination
- 5-year CBCT review (performed in Canada, uploaded to our portal, reviewed by the treating prosthodontist)
- 10-year written warranty active throughout
What "Remote" Actually Means
At Stunning Dentistry
The long-term maintenance plan above is not a courtesy; it is part of the treatment. Your year-one Zoom reviews are booked into the same clinical calendar as in-person cases. You are not a concluded file in month two, you are an ongoing clinical responsibility until the FMR has passed its first annual audit, and then every annual audit after that, for as long as the prosthesis is in your mouth. Continuity is the single biggest variable that separates long-term FMR outcomes from dental-tourism-averages. We do not hand you over. We stay with you.
| Timepoint | What Happens | Where |
|---|---|---|
| Week 1 home (post-trip 3) | Zoom check-in, hygiene photo review, healing assessment | Remote |
| Month 1 | Zoom consultation, prosthodontist review of intraoral photos | Remote |
| Month 3 | Zoom consultation + recommended hygienist visit in Canada | Remote + local |
| Month 6 | Zoom consultation, radiograph review (you upload a panoramic taken in Canada, we cover the cost) | Remote |
| Month 12 | First annual review, Zoom consultation, comprehensive clinical photo review, occlusal check, hygiene reinforcement | Remote |
If Something Goes Wrong After You're Home
We will be honest: no FMR is risk-free, and you are 8,000 km from the clinic. Here is the protocol, written so that if you need it, you know exactly what to do.
Step 1: Contact Your CRM Manager Immediately
- Single point of contact, 24/7/365, same contact across all trips and post-treatment years
- Phone, email, WhatsApp
- Average response time: under 30 minutes business hours, under 4 hours overnight
Step 2: Triage Within 24 Hours
- Same-day Zoom consultation with your lead prosthodontist
- Photo and intraoral video review
- Initial assessment: routine, urgent, or emergency
Step 3: Escalation Pathway
- Routine issues (minor chip, hygiene concern, small occlusal niggle), managed remotely, addressed at next planned visit or in-Canada hygienist appointment
- Urgent issues (persistent pain, suspected infection, screw failure, prosthesis fracture), referral to a vetted Canadian dentist or partner specialist for in-person assessment, with all clinical records shared and the visit reimbursable under warranty terms
- Emergencies (acute infection, major prosthetic fracture, suspected implant failure), immediate in-person Canadian assessment, expedited return travel for definitive management at Stunning Dentistry, flights and accommodation supported per the warranty schedule
Warranty Coverage in Plain Language
- Implants: 10-year written warranty against failure to integrate or premature loss (excluding wilful neglect or trauma)
- Prosthesis: documented warranty period covering material defects and structural failure
- Ceramic components: covered for defined period against chipping and material failure under normal function
- Repair fees: waived under warranty terms, only travel costs (in qualifying scenarios) and lab consumables apply
- Documentation: every FMR patient receives a written warranty document at definitive delivery, no verbal promises, no fine-print surprises
At Stunning Dentistry
Every component of this protocol exists because, across the last decade, we needed it. The Canadian-dentist referral network was built case by case after the third Toronto patient who needed after-hours screw retightening. The flight-supported return-for-revision clause was added after the first Montreal patient whose prosthesis fractured at month eight. We do not advertise these stories. They sit inside the warranty document, waiting to be invoked, written by experience rather than by marketing. If something goes wrong, the protocol is in place, you do not have to invent the response in a moment of panic.
Your Dental Tourism Safety Framework
If you are travelling internationally for an FMR, whether to us or to anyone else, these warnings are to be taken seriously. We would rather you trust the framework than trust a glossy advertisement.
Reject Any Clinic That
- Quotes a full mouth rehabilitation fee without seeing your CBCT or reviewing your full medical and dental history
- Guarantees a specific modality ("All-on-4" or "28 veneers") before clinical assessment
- Refuses to name the implant brand or ceramic material system
- Cannot show you 10-year clinical data for the implant or ceramic system being used
- Has no published or accessible warranty terms in writing
- Pressures you to commit on the day of inquiry or offers a "today-only" discount
- Cannot tell you the named clinician who will perform each phase
- Claims to complete a full mouth rehabilitation in one trip under 14 days
- Has no provisional testing phase in the proposed treatment plan
- Has no in-house CBCT, no in-house CAD-CAM, and outsources everything
- Has no structured remote follow-up protocol for international patients
- Mixes prices in a single figure you cannot break down line by line
- Has no independent reviews and no transparent complications data
What a Safe FMR Clinic Looks Like
- Specialist-led care (named prosthodontist + named surgical specialists)
- Multi-specialty team rounds on every complex case
- Internationally certified implant systems (Straumann, Nobel Biocare, Osstem, Dentsply, Zimmer)
- Named ceramic material systems with published track record (Zirkonzahn, IPS e.max, Lava Esthetic, Prettau Anterior)
- Hospital-grade sterilisation
- Published clinical outcomes
- Written warranty document
- Structured pre-op, intra-op, and post-op protocols
- Transparent itemised pricing
- A real, contactable post-op support system in Canada
- Willingness to tell you when their treatment is not the right fit for you
At Stunning Dentistry
We helped draft the framework above using the same criteria we would want applied to a family member choosing a clinic in any country. We are equally comfortable being rejected on our own test. If after reading this you are not convinced we pass every checkpoint, walk away. The international dental-tourism industry has grown in part because clinics have hidden behind glossy marketing. Our response is transparency over persuasion. We would rather you flew to a different clinic and had a great outcome than flew to us because you felt pressured.
Canadian Patient Stories
The patient experiences referenced here are paraphrased from consented patient testimony. Names and locations have been generalised for privacy. Clinical outcomes are accurate.
Rebecca, 54: Toronto
Gerry, 67: Vancouver
Amrita, 42: Calgary
Amrita's 30-month review showed intact restorations, no marginal staining, excellent periodontal health. She has referred her younger sister for a similar case.
Patient stories are consented and fact-checked against clinical records, edited only for privacy. We put prospective patients in direct touch with previous patients (with explicit permission) at the consultation stage.
At Stunning Dentistry
Rebecca, Gerry, and Amrita are not curated success stories. They are three of more than 280 Canadian FMR patients we have treated since the start of 2022. Their outcomes are typical, not exceptional, that is the point. We chose to publish them because their profiles reflect the three most common Canadian FMR presentations: the attrition-and-bruxism patient, the failing-bridge-plus-periodontal patient, and the congenital-defect patient. Whichever profile you most resemble, we have walked alongside someone like you before. The path is mapped; we can put you in touch.
Partner Dentists in Canada: Our Network Roadmap
Honesty first: as of April 2026, our in-Canada partner network is in active expansion. We do not pretend to have a clinic on every corner. Here is exactly where we stand and where we are going.
What Is Live Today
- Remote follow-up: 24/7 CRM, structured Zoom protocol, prosthodontist-led photo and radiograph review, operational now for every Canadian FMR patient
- Canadian hygienist roster: vetted hygienists in Toronto, Vancouver, Montreal, Calgary, and Edmonton who provide local maintenance visits with full clinical record sharing back to Stunning Dentistry
- Emergency referral pathway: confirmed referral relationships with select Canadian implant specialists and prosthodontists for urgent in-person assessment under our warranty terms
- FMR-specific support: Canadian hygienists briefed on sub-prosthetic cleaning for full-arch implant cases and ceramic-surface care for full-mouth crown rehabilitation
What Is Building Through 2026
- Formal partner-clinic agreements in Toronto, Vancouver, Montreal, and Calgary, clinics where in-person review and routine maintenance can happen as part of an integrated pathway
- Annual in-Canada clinical day visits by a Stunning Dentistry prosthodontist, on a rotating basis, for patient reviews and prospective consultations
- A published partner-clinic directory with credentials, scope of supported services, and patient feedback
- FMR-specific partnership criteria: partner clinics will hold explicit scope agreements covering routine FMR maintenance, hygiene support, and emergency triage
What This Means for You
- Full-quality clinical care across every trip
- Structured remote follow-up between trips and post-treatment
- A clear emergency pathway in Canada
- A network roadmap that expands in-person Canadian touchpoints through the year you are under treatment
We will not oversell what does not yet exist. The remote follow-up is excellent. The in-person Canadian footprint is growing. Both will be true on the day you book and both will be better six months later.
At Stunning Dentistry
We made a deliberate decision not to fabricate a Canadian "presence" we do not yet hold. Plenty of international dental operators list partner clinics that turn out to be phone forwarding numbers. We list only what is operational today and what is in active expansion this calendar year. When the formal partner-clinic agreements are signed, this section will be updated with named clinics, credentialled clinicians, and scope each one supports. Until then, the remote model carries the load, and it carries it well. We would rather under-promise and outperform than the reverse.
Clinics Near You: Which Stunning Dentistry Location Fits Your Trip
Stunning Dentistry operates from India's largest dental hospital footprint, with multiple locations equipped for Full Mouth Rehabilitation. The right destination for your trip depends on your origin city in Canada, your flight preference, and your case complexity.
Our FMR-Capable Locations
What Is the Same Across Every Location
What Differs
How We Help You Choose
Once you book the initial consultation, your CRM manager recommends the location best matched to your case complexity, flight preferences, and schedule. No extra fee for choosing one location over another, clinical fees are uniform across locations.
At Stunning Dentistry
One clinical governance framework, one SOP library, one warranty, one accountability chain. Whether you fly into Hyderabad, Delhi, Mumbai, or Bangalore, the implant brand is the same, the milling workflow is the same, the prosthodontist-implantologist pairing is the same, and the post-op pathway is the same. Every clinician treating you has been trained on the same internal protocol and audited against the same outcomes registry. A patient is never "downgraded" by choosing the city closer to their layover or their extended family. Uniformity is a deliberate engineering choice, not an accident of scale.
| Location | Access from Canada | Best For |
|---|---|---|
| **Hyderabad, Flagship Hospital** | Direct/1-stop from Toronto, Vancouver, Montreal, Calgary via Singapore/KL | Most complex cases, zygomatic, Tier 3 revisions, full international patient infrastructure |
| **Delhi NCR** | Direct/1-stop from major Canadian cities | Tier 1 and 2 cases; patients combining treatment with North India travel |
| **Mumbai** | 1-stop from major Canadian cities | Tier 1 and 2 cases; patients combining treatment with Mumbai or West India travel |
| **Bangalore** | 1-stop from Toronto, Vancouver | Tier 1 and 2 cases; patients with family or connections in South India |
Clinical References
This article references peer-reviewed research and authoritative texts from:
All clinical claims are sourced from indexed, peer-reviewed publications or recognised authoritative texts. No manufacturer-sponsored data has been presented as independent evidence.
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
How is full mouth rehabilitation different from smile design?
Smile design is aesthetic planning for visible teeth. FMR is functional, occlusal, structural, and aesthetic rebuilding of all teeth. Smile design is a component of aesthetic-led FMR but is not synonymous. An FMR patient might have smile design applied to the anterior 10–12 teeth within a broader 28-tooth rehabilitation.
Do I need my wisdom teeth out first?
Depends on their position and pathology. Impacted or partially erupted wisdom teeth are typically extracted before FMR begins because they compromise post-restorative maintenance and can harbour infection near distal abutments. Fully erupted, functional wisdom teeth are often kept.
Can I eat normally during the provisional phase?
Yes, with caution for the first 2–4 weeks while the soft tissue adapts. The PMMA provisional is designed to restore function; ice and bones are off-limits, but steak, vegetables, fruit, and bread are on the menu.
Is my case fixed-implant or tooth-supported?
The honest answer: it depends on the CBCT, the periodontal chart, the endodontic status of remaining teeth, your bruxism history, and your preference. We assess all five variables in the diagnostic workup and present the case for each modality at consultation. You see the reasoning, not just the recommendation.
How many visits will I need at Stunning Dentistry?
Tier 1: two trips. Tier 2: three trips. Tier 3: three to four trips. The specific schedule is defined in your tier assignment at the end of the first consultation.
What lab materials will you use on my case?
Position-by-position, documented in the treatment plan. Typically monolithic zirconia (3Y-TZP) for posterior load-bearing, layered zirconia or lithium disilicate (IPS e.max) for anterior aesthetics, PEKK for implant bar substructures where relevant. We do not use budget ceramic systems on FMR cases.
What splint will I wear?
Usually a full-coverage hard acrylic Michigan splint fitted at the end of the FMR. For diagnostic and pre-treatment phases, a Tanner splint or NTI-style anterior deprogrammer may be used. The splint type is matched to your bruxism profile and documented in the plan.
What about my TMJ symptoms?
TMJ symptoms are not a contraindication to FMR. Often FMR resolves TMJ symptoms because the redesigned occlusion relieves the loads that drove the symptoms. If your TMJ is symptomatic, a pre-treatment TMJ assessment is performed, splint therapy is used diagnostically, and only after symptoms are stable or clearly addressable does definitive restoration proceed.
What is your refurbishment and remake policy?
Minor ceramic chips, stain accumulation, and glaze wear, refurbished at the annual review, no additional fee. Full crown remake (single unit), covered under warranty in defined scenarios (material defect, prosthetic screw failure, documented premature fracture). Full prosthesis remake, rare; when it happens, the scope of warranty coverage is defined in your written warranty document at delivery.
What if a tooth fails mid-treatment?
Contingency is built into the plan. A strategic tooth that unexpectedly fails during the provisional phase is extracted and the slot converted to an implant or a pontic. For tooth-supported FMR cases, we build an "acceptable loss margin" into the plan, which teeth can be sacrificed without rebuilding the entire plan, and which are load-critical. You see this in the treatment plan upfront.
Can I combine FMR with orthognathic surgery?
Yes. Orthognathic (jaw) surgery is combined with FMR in selected cases, severe skeletal discrepancies, class III bites with tooth wear, asymmetric jaw growth. The coordination adds to trip count and duration but is highly effective when indicated. Our oral and maxillofacial surgery team leads the orthognathic phase.
Will I look different after FMR?
Usually yes, in a restorative sense. Lip support is regained. VDO is increased. The lower third of the face is restored to its native proportions. The change is flattering and typically makes patients look 5–10 years younger, not because of cosmetic artifice but because of structural restoration.
What happens if I stop attending maintenance?
Failure rates increase substantially. Published mechanical complication rates rise from 15–20 per cent (with maintenance) to 35–50 per cent (without). Peri-implantitis, periodontal progression, and screw loosening are the three major non-maintenance failure modes.
Do I need to stop smoking?
Strongly recommended. Smoking doubles marginal bone loss around implants and slows soft tissue healing. For implant-dependent FMR cases, smoking cessation for at least 8 weeks pre-surgery and ideally indefinitely post-surgery is our standard requirement.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.