CBCT Dental ScanningWhat It Measures, What It Reveals, and Why It Precedes Every Implant Plan
- CBCT scanning is the imaging technology that converted implant dentistry from an anatomical estimate into a measurable surgical plan.
Before CBCT, a surgeon planning implant placement worked from two-dimensional panoramic radiographs that could show bone height but not bone width, and showed the inferior alveolar nerve as a flat shadow rather than a three-dimensional structure.
Overview
What is CBCT dental scanning?
> Cone Beam Computed Tomography (CBCT) is a three-dimensional radiographic imaging technique that produces volumetric data of the jaw, teeth, and surrounding bone. Unlike a flat dental X-ray, it reveals bone width, height, density, sinus anatomy, and nerve canal position, the measurements that determine whether and how implants can be placed.
CBCT scanning is the imaging technology that converted implant dentistry from an anatomical estimate into a measurable surgical plan. Before CBCT, a surgeon planning implant placement worked from two-dimensional panoramic radiographs that could show bone height but not bone width, and showed the inferior alveolar nerve as a flat shadow rather than a three-dimensional structure. The consequences of that information gap, nerve damage, implant placement into insufficient bone, sinus perforations, were not rare events.
Cone beam CT provides three-dimensional data essential for accurate implant planning, including bone volume, bone density, proximity to vital structures, and sinus floor topography. Its use is recommended for complex implant cases and for full-arch rehabilitation.
At Stunning Dentistry, we require CBCT imaging for every full-arch implant case before treatment planning begins. For single-implant cases, CBCT is recommended where the clinical examination raises any question about bone volume, nerve proximity, or sinus involvement. Treatment planning without three-dimensional imaging is not a service we offer for complex cases, it is a risk we are not willing to take on your behalf.
| Imaging Type | Dimensions | Bone Width | Bone Density | Nerve Position | Sinus Anatomy |
|---|---|---|---|---|---|
| Periapical X-ray | 2D | No | No | Approximate | No |
| Panoramic X-ray | 2D | No | Limited | Shadow only | Limited |
| CBCT | 3D volumetric | Yes | Yes (HU value) | Precise | Yes |
| Medical CT | 3D volumetric | Yes | Yes | Yes | Yes |
Questions about this procedure?
What Is CBCT Dental Scanning?
Cone Beam Computed Tomography is a radiographic imaging technique in which an X-ray source and detector rotate around the patient's head in a single pass, capturing multiple two-dimensional projections that are reconstructed by software into a three-dimensional volumetric dataset. The name refers to the cone-shaped beam geometry, which differs from the fan-beam geometry of medical CT scanners. This cone beam geometry reduces radiation dose and allows a compact, chair-side unit, but limits soft tissue contrast compared with medical CT.
CBCT produces isotropic voxels as small as 0.076mm, enabling sub-millimetre precision in bone measurement. This resolution is sufficient for implant site analysis, orthodontic assessment, endodontic anatomy, and surgical planning of complex extractions.
At Stunning Dentistry, we use full-arch field-of-view CBCT for implant planning, capturing both arches and the relevant sinus anatomy in a single scan where indicated. The DICOM data is reviewed by the treating clinician in planning software, not delegated to a radiologist's report alone, because the clinical interpretation for implant planning requires the surgeon's specific knowledge of the intended implant positions.
| Feature | Description |
|---|---|
| Scan duration | 10–40 seconds of rotation |
| Total appointment | 15–30 minutes including positioning |
| Data format | DICOM (universal, transferable) |
| Voxel size (typical dental CBCT) | 0.076–0.3mm isotropic |
| Planning software compatible | coDiagnostiX, Simplant, Nobel Clinician, 3Shape Implant Studio |
| Output views | Axial, coronal, sagittal cross-sections + 3D reconstruction |
Ready to discuss your options?

How CBCT Differs from a Standard Dental X-Ray
Standard dental radiographs, panoramic and periapical, project three-dimensional anatomy onto a two-dimensional plane. The resulting image is a shadow: a compression of bone, roots, and nerves into a flat representation where structures overlap and the third dimension (bone width, buccal-lingual depth) is invisible. This two-dimensional constraint is acceptable for diagnosing caries, assessing periodontal bone levels, or evaluating a single root canal. It is not acceptable for planning the precise three-dimensional position of a titanium implant in living bone.
Panoramic radiography systematically distorts image dimensions by 20–30% due to geometric magnification, and cannot represent bone width or three-dimensional nerve anatomy. Decisions based solely on panoramic imaging carry a documented risk of anatomical misinterpretation in implant surgery.
At Stunning Dentistry, we do not use panoramic radiography as the sole imaging basis for implant planning. Panoramic images are useful as an initial survey of the dentition, they give us the overview. CBCT gives us the measurement. Both have their function; the panoramic image does not replace the three-dimensional data that implant placement requires.
| Measurement | Panoramic X-ray | CBCT |
|---|---|---|
| Bone height | Approximate (distorted) | Precise (sub-mm) |
| Bone width | Not visible | Precise (sub-mm) |
| Bone density | Not measurable | Hounsfield units (HU) |
| Nerve canal position | 2D shadow, approximate | 3D tract, precise |
| Sinus floor topography | Flat projection only | Full 3D anatomy |
| Implant angulation planning | Not possible | Fully plannable |
| Surgical guide derivation | Not possible | Direct digital workflow |
Curious about costs and timelines?
What a CBCT Scan Measures
A dental CBCT scan produces volumetric data that the clinician interrogates in cross-sectional slices in three planes: axial (top-down), coronal (front-back), and sagittal (side-side). From these slices, the following measurements are extracted for each planned implant site: bucco-lingual bone width (is the ridge wide enough for the implant diameter plus 1.5mm of peripheral bone on each side?); apico-coronal bone height (is there enough vertical bone before the inferior alveolar nerve or sinus floor?); bone density by Hounsfield Unit value (Type I through IV bone, Lekholm and Zarb classification); and the precise three-dimensional position of the inferior alveolar nerve canal in the mandible.
Bone density measured by CBCT using Hounsfield units is a validated predictor of implant primary stability. Type IV bone (HU <150) is associated with lower insertion torque values and increased short-term implant failure risk compared with Type I–III bone.
At Stunning Dentistry, we walk every full-arch patient through their CBCT data during the treatment planning appointment. The planned implant positions are plotted on the scan, the relevant measurements are recorded in the treatment plan, and the bone quality classification for each site is documented before any surgical scheduling occurs.
| CBCT Measurement | Clinical Relevance | Minimum Threshold |
|---|---|---|
| Bucco-lingual bone width | Implant diameter + 1.5mm wall each side | ≥6mm for 3.75mm implant |
| Apico-coronal bone height (mandible) | Distance to inferior alveolar nerve | ≥2mm safety margin below apex |
| Apico-coronal bone height (maxilla) | Distance to sinus floor | ≥1mm residual floor or sinus lift indicated |
| Bone density (Hounsfield Units) | Primary stability prediction | Type I–III preferred; Type IV = modified protocol |
| Nerve canal position | Avoid surgical trauma | 3D tracing, not 2D estimate |
| Sinus pneumatisation | Determines sinus lift need | Floor height above alveolar crest |
Want a personalised treatment plan?

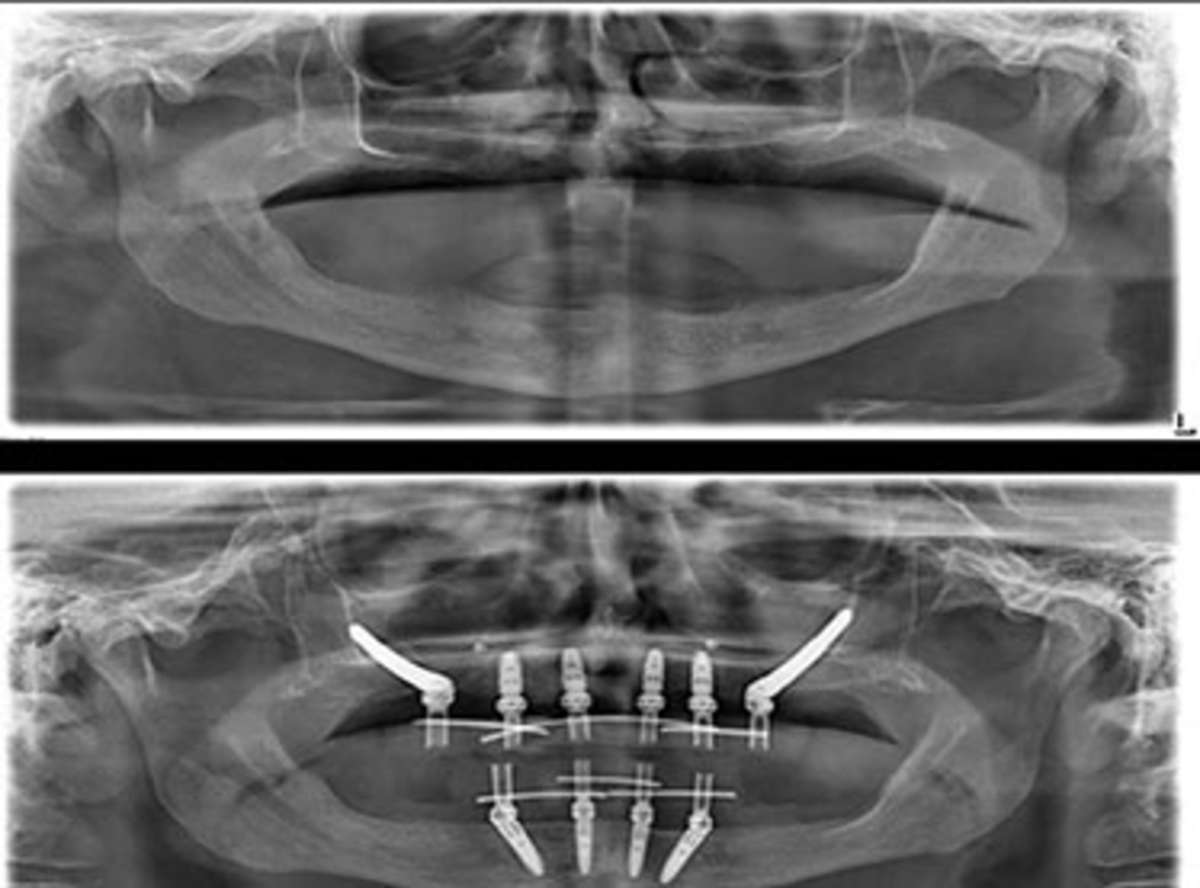
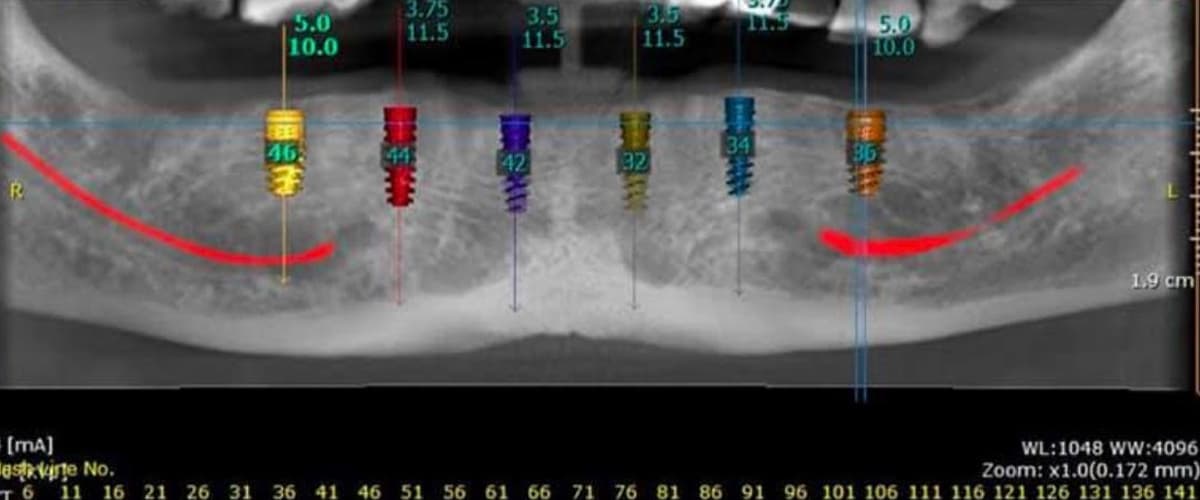
How the Scan Is Used in Implant Planning
The CBCT DICOM file is imported into implant planning software where the surgeon places virtual implants into the three-dimensional bone reconstruction. Each implant can be adjusted in position, angulation, depth, and diameter until it satisfies the bone volume requirements, avoids vital structures, and is aligned with the planned prosthetic outcome. This virtual placement is not the final surgical decision, it is the planning tool that makes the surgical decision informed rather than estimated.
Virtual implant planning using CBCT-derived three-dimensional models allows pre-surgical determination of implant position with documented accuracy when converted to a physical surgical guide. The mean deviation between planned and actual position in full-arch guided cases is 1.0–1.5mm at the implant apex.
At Stunning Dentistry, we use coDiagnostiX software for implant planning on full-arch cases. The planned positions are reviewed by the surgical and prosthodontic team together before the surgical guide is fabricated. The prosthetic outcome drives the implant positions, not the available bone alone, because an implant placed in the wrong position for the planned prosthesis is a surgical success that fails the patient.
| Planning Software Step | Output |
|---|---|
| DICOM import + segmentation | Three-dimensional bone model |
| Virtual implant placement | Position, angulation, depth, diameter for each fixture |
| Prosthetic-driven positioning | Implant axis aligned with planned crown/bridge |
| Safety margin verification | Nerve, sinus, adjacent root clearance confirmed |
| Surgical guide design | Tooth-supported, mucosa-supported, or bone-supported guide |
| Guide fabrication | 3D-printed surgical-grade resin with metal sleeves |
Questions about this procedure?

Radiation Dose and Safety
CBCT radiation dose is substantially lower than medical CT scanning and is calibrated to the clinical question. A full-arch dental CBCT delivers an effective dose of approximately 40–200 microsieverts (µSv) depending on the field of view, voxel size, and machine settings. For comparison, a medical head CT delivers approximately 1,000–2,000 µSv; a transatlantic flight delivers approximately 50–80 µSv from cosmic radiation; and annual background radiation exposure in most countries is 2,000–3,000 µSv. The radiation from a full-arch CBCT is therefore comparable to one to four days of natural background exposure.
The radiation dose from dental CBCT, when optimised using appropriate field of view selection and exposure parameters, is within the range of accepted dental radiographic procedures. The benefit-to-risk ratio is strongly positive for clinically indicated cases.
At Stunning Dentistry, we select the smallest field of view appropriate to the clinical question, a single quadrant scan where only one area is being assessed, a full-arch scan where multiple implant positions are being planned, and a maxillofacial scan only where sinus anatomy or orthognathic assessment requires it. Dose optimisation is not optional; it is part of the imaging protocol.
| Imaging Source | Effective Dose (µSv) | Equivalent to |
|---|---|---|
| Periapical X-ray (single) | 1–8 | Hours of background radiation |
| Panoramic X-ray | 4–30 | 1–2 days background |
| Dental CBCT (small FOV) | 20–50 | 1–3 days background |
| Dental CBCT (full arch) | 40–200 | 3–12 days background |
| Medical head CT | 1,000–2,000 | 3–6 months background |
| Transatlantic flight | 50–80 | ~3 days background |
| Annual background (UK/Canada) | ~2,400 | , |
Ready to discuss your options?

When CBCT Scanning Is Required vs Optional
CBCT scanning is not required for every dental procedure, but for implant surgery it transitions from optional to required based on case complexity. The threshold is defined by the clinical consequences of planning from two-dimensional data: when the gap between the panoramic image and the three-dimensional reality could result in nerve injury, sinus perforation, or implant placement in insufficient bone, CBCT is required. For straightforward single implants in visually adequate bone with no anatomical concerns, the risk-benefit calculation may favour panoramic imaging alone, but this is a clinician decision, not a patient preference.
CBCT is recommended for all full-arch implant rehabilitation cases, for implants in the posterior mandible where the inferior alveolar nerve position is critical, for maxillary posterior implants where sinus anatomy is uncertain, and for any site where previous imaging or examination raises doubt about bone volume.
At Stunning Dentistry, our CBCT policy is: required for all full-arch cases, all zygomatic implant cases, all cases requiring bone grafting assessment, and all single-implant cases where clinical examination cannot confirm adequate bone volume. We do not substitute clinical impression for measurement where measurement is achievable.
| Clinical Scenario | CBCT Required | Rationale |
|---|---|---|
| Full-arch implant rehabilitation (All-on-4/6) | Yes, mandatory | Bone volume, tilt planning, nerve/sinus mapping |
| Zygomatic implants | Yes, mandatory | Zygomatic arch geometry, sinus health |
| Posterior mandible single implant | Recommended | Inferior alveolar nerve position |
| Posterior maxilla single implant | Recommended | Sinus floor height |
| Anterior single implant, adequate bone | Optional | Panoramic may suffice if no concerns |
| Bone grafting assessment | Recommended | Volume quantification |
| Implant in grafted site | Required | Graft integration assessment |
Curious about costs and timelines?
What the Scan Cannot Tell You
CBCT imaging reveals hard tissue: bone, tooth roots, calcified structures, and airway anatomy. It does not image soft tissue with clinical precision. The health of the gingiva, the state of the periodontal ligament, the thickness of the attached keratinised tissue at implant sites, the presence of active infection in bone that has not yet shown radiographic change, none of these are reliably assessed by CBCT. A patient can have a technically excellent CBCT scan showing adequate bone volume and still have active periodontal disease that contraindicates implant placement.
CBCT cannot replace clinical periodontal examination, probing, or soft tissue assessment. Imaging findings must always be interpreted in the context of a full clinical examination. CBCT showing apparently adequate bone in the presence of unmanaged periodontitis does not confirm implant candidacy.
At Stunning Dentistry, CBCT review is one step within a multi-stage assessment protocol. The scan findings are interpreted alongside periodontal charting, medical history screening, occlusal analysis, and the patient's functional goals. An implant plan is not confirmed until all components of that assessment are complete.
| CBCT Shows | CBCT Does Not Show |
|---|---|
| Bone volume (width, height, density) | Gum health or periodontal attachment |
| Nerve canal position | Active soft tissue infection |
| Sinus anatomy | Occlusal force distribution |
| Root positions of adjacent teeth | Bite force or parafunction |
| Calcified lesions, cysts (if mineralised) | Early-stage osteonecrosis |
| Existing implant positions | Soft tissue thickness at implant site |
Want a personalised treatment plan?
Risk and Limitations
CBCT imaging carries a radiation dose, small, but not zero, and decisions about when to scan should account for cumulative exposure, particularly in younger patients or those requiring serial imaging. Beyond dose, CBCT has technical limitations: image artefacts from metal restorations (amalgam, crowns, existing implants) can obscure adjacent bone and reduce measurement reliability in the affected region. Motion artefacts from patient movement during the scan degrade image quality and may require rescanning. And CBCT bone density measurement (Hounsfield units) is less standardised across machines than in medical CT, meaning density values should be interpreted with awareness of the specific machine's calibration.
Metal artefact scatter from existing restorations significantly reduces CBCT diagnostic accuracy in the immediate vicinity of metal structures. For patients with multiple existing implants or large metal restorations, image quality limitations should be discussed before planning critical measurements in affected areas.
At Stunning Dentistry, we review CBCT image quality before using data for surgical planning. If artefact compromises the measurement accuracy at a critical site, we document the limitation and apply a conservative safety margin or request additional imaging. We do not proceed with a surgical plan based on compromised imaging data.
| Limitation | Clinical Impact | Management |
|---|---|---|
| Metal artefact scatter | Reduced bone measurement accuracy near metal | Conservative planning margins; note in record |
| Motion artefact | Blurred image, reduced resolution | Rescan if critical measurements affected |
| Soft tissue invisibility | Gum health not assessable | Supplement with clinical examination |
| Bone density calibration variance | HU values vary between machines | Relative classification; not absolute |
| Field of view constraint | Small FOV misses adjacent anatomy | Select appropriate FOV for case |
Questions about this procedure?
When CBCT Is Not Indicated
CBCT is not appropriate for every dental clinical question. Routine caries detection, periapical pathology assessment on single teeth, periodontal bone level measurement, and orthodontic treatment monitoring do not routinely require CBCT, two-dimensional imaging is sufficient, the dose is lower, and the three-dimensional data adds no diagnostic value. Exposing a patient to CBCT radiation for a clinical question answerable by a periapical X-ray is not justified by any risk-benefit analysis.
The ALARA principle (As Low As Reasonably Achievable) requires that radiation exposure be minimised while achieving the diagnostic objective. CBCT is not indicated where two-dimensional radiography provides equivalent diagnostic information at substantially lower dose.
At Stunning Dentistry, we do not perform CBCT as a screening or marketing tool. Each scan request is clinically justified, the field of view is matched to the clinical question, and the findings are integrated into a documented treatment plan. If a panoramic image adequately answers the clinical question for a simple case, that is the imaging we use.
| Scenario | Indicated Imaging | Reason CBCT Not Needed |
|---|---|---|
| Routine caries check | Bitewing X-rays | 2D sufficient; lower dose |
| Single periapical assessment | Periapical X-ray | 2D sufficient |
| Orthodontic monitoring (stable case) | Cephalometric + OPG | 2D sufficient for most |
| Periodontal bone level assessment | Periapical series | 2D sufficient |
| Simple single implant, adequate bone | Panoramic + periapical | 2D planning viable |
| Full-arch implant planning | CBCT required | 3D bone data essential |
Ready to discuss your options?

Cost Logic
CBCT scanning in Canada and India uses the same international machine manufacturers (NewTom, i-CAT, Planmeca, Carestream). The DICOM output is standardised, a scan performed in Canada is readable by Stunning Dentistry's planning software, and vice versa.
| Provider | CBCT Scan Cost (CAD) | Notes |
|---|---|---|
| Stunning Dentistry (India) | $300–500 | Full-arch field of view; DICOM file provided; included in full-arch treatment planning |
| Canadian dental clinic | $400–800 | Varies by clinic and field of view; DICOM usually provided on request |
| Canadian hospital radiology | $600–1,200 | Medical CT; higher dose; often not required for implant planning |
| Canadian oral radiology specialist | $350–700 | Dedicated CBCT clinic; DICOM and radiology report |
Curious about costs and timelines?
CBCT vs Panoramic vs Periapical: Comparison
| Feature | Periapical | Panoramic (OPG) | CBCT |
|---|---|---|---|
| Dimensions | 2D | 2D | 3D volumetric |
| Field of view | Single tooth/region | Full dentition | Variable (small to full arch) |
| Bone width | Not visible | Not visible | Measurable |
| Bone density | Not measurable | Limited | Hounsfield units |
| Nerve canal (3D) | No | Shadow only | Precise 3D tract |
| Sinus anatomy | No | Partial | Full 3D |
| Implant planning | Limited | Survey only | Full |
| Surgical guide design | Not possible | Not possible | Direct digital workflow |
| Radiation dose | 1–8 µSv | 4–30 µSv | 40–200 µSv |
| Cost (CAD, Canada) | $30–80 | $80–180 | $350–800 |
Want a personalised treatment plan?
Common Misunderstandings About CBCT
The most common misunderstanding about CBCT is that it is equivalent to a medical CT scan in dose and complexity. It is not. Medical CT uses a fan-beam geometry, higher milliamperage, and continuous rotation to achieve excellent soft tissue contrast, at a substantially higher radiation dose than dental CBCT. A dental cone beam unit is specifically engineered for hard tissue imaging of a small anatomical field, with a dose profile that is an order of magnitude lower than head CT and comparable to a small number of panoramic radiographs. The two should not be conflated when assessing risk.
Patient concerns about dental CBCT radiation often reflect a confusion between dental and medical CT. The effective dose from dental CBCT is 5–50 times lower than medical head CT. When contextualised against natural background radiation, dental CBCT represents a low and clinically justified exposure.
At Stunning Dentistry, we regularly receive CBCT DICOM files from Canadian patients before their travel appointment. Pre-consultation planning from your Canadian scan allows us to identify any additional imaging needs, prepare a preliminary treatment plan, and use your first in-clinic appointment for clinical examination and plan confirmation rather than starting the imaging process from scratch.
| Myth | Reality |
|---|---|
| CBCT is the same as a medical CT scan | Medical CT dose is 5–50× higher; different geometry and indication |
| The scan is used to upsell treatment | CBCT changes treatment plans, sometimes reduces scope, not always increases |
| CBCT is only needed for complex cases | Required for all full-arch and zygomatic cases regardless of apparent complexity |
| Any dental clinic can interpret CBCT for implants | Implant-specific software interpretation requires surgical/prosthetic clinical knowledge |
| I have to get the scan in India | A Canadian CBCT DICOM file is transferable and usable internationally |
Questions about this procedure?
People Also Ask
Is CBCT radiation dangerous for dental scanning?
Yes. CBCT data is stored in the universal DICOM format, readable by all major implant planning software worldwide. A scan performed at any Canadian dental or radiological clinic can be transferred electronically to Stunning Dentistry for pre-consultation treatment planning, allowing a detailed implant plan to be prepared before you travel.
Ready to discuss your options?
Ask Your Doctor
Before your CBCT scan or implant planning consultation, ask:
- What field of view are you using for my scan, and why?
- Will I receive a copy of the DICOM file from my scan?
- Which software will you use to plan my implant positions from the scan data?
- Will the surgeon reviewing the scan also be performing my surgery?
- What bone measurements are required for the implants I'm having placed, and does my scan meet them?
- If my scan shows insufficient bone, what are the options, grafting, different implant type, or modified position?
Curious about costs and timelines?
Want a personalised treatment plan?
For Canadian Patients: CBCT Planning from Canada
Canadian patients can have CBCT scanning performed at any dental radiology clinic, oral and maxillofacial radiology specialist, or dental clinic with a CBCT unit before travelling to India. The cost at a Canadian clinic ranges from CAD $350–800 depending on field of view and whether a radiologist's report is included. At Stunning Dentistry, CBCT scanning is included in full-arch implant treatment planning costs, or available as a standalone service for CAD $300–500.
At Stunning Dentistry, our Dental Angel handover protocol includes providing you with your complete CBCT DICOM file at the end of treatment. This file travels back to Canada with you and is transferable to your Canadian dentist for continuity of care. Your Canadian dentist does not need special equipment to view the data, DICOM viewer software is available free of charge, and your CBCT data includes the complete three-dimensional record of your bone anatomy and implant positions at the time of treatment.
Questions about this procedure?
CAD Cost Table
| Service | Stunning Dentistry (India) | Canadian Dental Clinic | Canadian Oral Radiology Specialist |
|---|---|---|---|
| Full-arch CBCT scan | CAD $300–500 | CAD $400–800 | CAD $350–700 |
| Implant planning consultation (with CBCT review) | Included in treatment | CAD $200–500 | N/A |
| Surgical guide fabrication (from CBCT data) | Included in full-arch treatment | CAD $800–1,500 | N/A |
| DICOM file copy | Included | Usually provided on request | Included |
| Pre-consultation virtual planning (from your Canadian scan) | No charge | N/A | N/A |
Ready to discuss your options?
Pre-Travel Checklist for Canadian Patients
"@context": "https://schema.org",
"@type": "FAQPage",
"@type": "Question",
"name": "Is CBCT radiation dangerous for dental scanning?",
"acceptedAnswer": {
"@type": "Answer",
"text": "CBCT dental scanning delivers substantially less radiation than a medical CT scan. A full-arch dental CBCT delivers approximately 40–200 microsieverts, equivalent to 3–12 days of natural background radiation. When CBCT is clinically indicated for implant planning, the diagnostic benefit significantly outweighs the radiation risk."
"@type": "Question",
"name": "Do I need a CBCT scan before dental implants?",
"acceptedAnswer": {
"@type": "Answer",
"text": "For full-arch rehabilitation (All-on-4, All-on-6, zygomatic implants), CBCT is required, it is the only imaging modality that reveals bone volume, density, sinus floor height, and inferior alveolar nerve position in three dimensions. For single implants in straightforward cases, CBCT is recommended but clinical judgement applies."
"@type": "Question",
"name": "What does CBCT show that a dental X-ray does not?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Standard dental X-rays are two-dimensional. CBCT produces three-dimensional volumetric data: bone width and height at each implant site, cortical bone thickness, cancellous bone density, sinus pneumatisation, and the precise three-dimensional position of the inferior alveolar nerve canal, none of which are measurable on a 2D radiograph."
"@type": "Question",
"name": "How long does a CBCT dental scan take?",
"acceptedAnswer": {
"@type": "Answer",
"text": "The scanning rotation takes 10–40 seconds. The total appointment including positioning and initial review is 15–30 minutes. DICOM data processing and treatment planning analysis by the clinician takes 1–3 hours of clinical time subsequently."
"@type": "Question",
"name": "Can I get a CBCT scan done in Canada and bring it to India?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Yes. CBCT data is stored in the universal DICOM format, readable by all major implant planning software worldwide. A scan performed at any Canadian dental or radiology clinic can be transferred electronically to Stunning Dentistry for pre-consultation treatment planning before you travel."
"@type": "MedicalProcedure",
"name": "CBCT Dental Scanning",
"procedureType": "Diagnostic Imaging",
"description": "Cone Beam Computed Tomography (CBCT) is a three-dimensional radiographic imaging technique used in implant dentistry to measure bone volume, density, sinus anatomy, and nerve canal position before surgical planning.",
"bodyLocation": "Jaw and maxillofacial structures",
"@type": "MedicalOrganization",
"name": "Stunning Dentistry",
"url": "https://stunningdentistry.com"
"@type": "Physician",
"name": "Dr. Priyank Sethi",
"description": "MDS Prosthodontics, Ph.D. in Dentistry, Founder & CEO, Stunning Dentistry",
"medicalSpecialty": "Prosthodontics",
"@type": "MedicalOrganization",
"name": "Stunning Dentistry"
Medically Reviewed
Reviewed by: Dr. Priyank Sethi, MDS Prosthodontics, Ph.D. in Dentistry
Last Updated: May 2025
| Item | Details |
|---|---|
| CBCT DICOM file (if scanned in Canada) | Request from your Canadian dental or radiology clinic before travel |
| Panoramic X-ray (OPG) | Bring most recent, if available |
| Dental records summary | Existing restorations, extractions, implants, graft history |
| Medical history form | Completed before arrival; medications, systemic conditions, allergies |
| Medication list | Including bisphosphonates, anticoagulants, immunosuppressants, diabetes medication |
| Travel insurance documentation | Medical coverage confirmed for duration of treatment |
| Canadian dentist contact | Name and contact for Dental Angel handover coordination |
| Flight timing | Plan minimum 48 hours post-scan before flying if scan is day-of-arrival |
| Accommodation confirmed | Near clinic for follow-up appointments |
| Emergency contact registered | With clinic coordinator before departure |
Curious about costs and timelines?
Clinical References
- Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R. Cone beam computed tomography in implant dentistry: a systematic review focusing on guidelines, indications, and radiation dose risks. *International Journal of Oral & Maxillofacial Implants*. 2014;29(Suppl):55–77.
- Harris D, Buser D, Dula K, et al. EAO guidelines for the use of diagnostic imaging in implant dentistry 2011. A consensus workshop organized by the European Association for Osseointegration at the Medical University of Warsaw. *Clinical Oral Implants Research*. 2012;23(11):1243–53.
- Guerrero ME, Jacobs R, Loubele M, Schutyser F, Suetens P, van Steenberghe D. State-of-the-science on cone beam CT imaging for preoperative planning of implant placement. *Clinical Oral Investigations*. 2006;10(1):1–7.
- Dreiseidler T, Mischkowski RA, Neugebauer J, Ritter L, Zöller JE. Comparison of cone-beam imaging with orthopantomography and computerized tomography for assessment in presurgical implant dentistry. *International Journal of Oral & Maxillofacial Implants*. 2009;24(2):216–25.
- Pauwels R, Beinsberger J, Collaert B, et al. Effective dose range for dental cone beam computed tomography scanners. *European Journal of Radiology*. 2012;81(2):267–71.
- Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. *International Journal of Oral & Maxillofacial Implants*. 2014;29(Suppl):25–42.
- Cassetta M, Stefanelli LV, Pacifici A, Pacifici L, Barbato E. How accurate is CBCT in measuring bone density? A comparative CBCT-CT in vitro study. *Clinical Implant Dentistry and Related Research*. 2014;16(4):471–8.
- European Commission. Radiation protection No. 172: Cone beam CT for dental and maxillofacial radiology, evidence-based guidelines. Luxembourg: Publications Office of the European Union; 2012.
Want a personalised treatment plan?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
Can I have CBCT scanning if I'm pregnant?
CBCT should be deferred in pregnancy unless there is an urgent clinical need that cannot wait. While dental CBCT doses are low, elective radiographic imaging is generally deferred during pregnancy as a precautionary principle. Emergency imaging decisions should involve the patient's obstetrician.
How often do I need CBCT imaging for implant follow-up?
CBCT is generally not required for routine implant follow-up. Periapical radiographs are sufficient for monitoring peri-implant bone levels annually. CBCT would be re-indicated if implant complications arise that require three-dimensional assessment, infection, suspected nerve involvement, or evaluation of bone loss extent.
My panoramic X-ray shows I have enough bone. Do I still need CBCT?
A panoramic X-ray shows bone height but not bone width. A ridge that appears tall on a panoramic image may be very narrow, a finding only visible on CBCT cross-section. For full-arch cases particularly, panoramic imaging cannot confirm adequacy of bone volume. CBCT is still required.
Can two different CBCT machines read each other's DICOM files?
Yes. DICOM is an internationally standardised data format. Any CBCT DICOM file can be imported into any compatible implant planning software regardless of which machine produced it. Image resolution and voxel size vary by machine and settings, but the file format is universally compatible.
What happens after the CBCT scan?
The DICOM data is imported into implant planning software. Your surgeon or prosthodontist reviews the scan, places virtual implants at the planned positions, verifies bone volume and safety margins, and generates a treatment plan. If surgical guides are being fabricated, the planned implant positions are exported to guide design software. You will typically receive a presentation of your CBCT findings and proposed treatment at your planning consultation.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










