Computer-Guided Implant SurgeryHow CBCT Data, Software Planning, and a Surgical Guide Replace Freehand Estimation
- Computer-guided implant surgery is not a procedure type, it is a planning and execution methodology applied to implant placement.
The implant itself is identical whether it is placed freehand or guided.
Overview
What is computer-guided implant surgery?
> Computer-guided implant surgery uses three-dimensional CBCT imaging data and planning software to create a physical surgical guide that constrains the drill to a pre-planned implant position and angulation. It converts the surgeon's digital plan into a physical instrument, reducing the gap between intended and actual implant placement.
Computer-guided implant surgery is not a procedure type, it is a planning and execution methodology applied to implant placement. The implant itself is identical whether it is placed freehand or guided. What changes is the precision of its position. In full-arch rehabilitation, where the angulation and position of each implant determines the long-term biomechanics of the prosthesis, the gap between planned and actual position has measurable clinical consequences: a 2mm deviation at the implant apex can shift a cantilever length from acceptable to fracture-risk territory.
Computer-guided implant surgery using CBCT-derived surgical guides achieves a mean apex deviation of 1.2–1.5mm compared with 2.0–2.5mm for experienced freehand surgeons. The advantage is most pronounced in full-arch cases, posterior mandible positions, and anterior aesthetic zones where angulation is critical.
At Stunning Dentistry, we use computer-guided implant placement for all full-arch cases, All-on-4, All-on-6, and zygomatic, as standard of care. For single implants where adjacent anatomy is complex, posterior nerve proximity is a concern, or the aesthetic demand is high, guided placement is used selectively based on clinical judgment. The surgical guide is fabricated from your CBCT data and your specific planned implant positions, not from a generic template.
| Guided Surgery Feature | Description |
|---|---|
| Data source | Patient's CBCT DICOM file |
| Planning software | coDiagnostiX, Simplant, Nobel Clinician, 3Shape |
| Guide material | Surgical-grade 3D-printed resin |
| Guide type | Tooth-supported, mucosa-supported, or bone-supported |
| Metal sleeves | Constrain drill to planned trajectory |
| Output accuracy (apex, mean) | 1.0–1.5mm deviation from planned position |
Questions about this procedure?
What Is Computer-Guided Implant Surgery?
Computer-guided implant surgery describes the use of three-dimensional imaging data, typically CBCT, to plan implant positions digitally, then translate that plan into a physical surgical guide that constrains the drill at the time of surgery. The guide is a patient-specific appliance that fits over the existing teeth, the edentulous ridge mucosa, or the exposed alveolar bone, and contains metal drill sleeves oriented exactly to the planned implant trajectories. When the surgeon drills through the sleeve, the drill can only follow the planned path, it cannot deviate in angulation or, with depth-stop accessories, in depth.
Computer-aided implant surgery systems provide a reproducible link between virtual treatment planning and surgical execution. The clinical benefit is reduction in positional deviation, particularly in full-arch cases where the cumulative effect of multiple implant positions determines prosthetic outcome.
At Stunning Dentistry, we review every guided surgery plan with both the surgeon and the prosthodontist before the guide is fabricated. The prosthetic outcome drives the implant positions, the planned bridge or arch prosthesis defines where the implants must be, and the plan is evaluated against both the bone anatomy and the restorative geometry simultaneously. An implant that satisfies bone requirements but produces an unrestorable prosthetic situation is not an acceptable plan.
| Component | Role in Guided Surgery |
|---|---|
| CBCT scan | Provides three-dimensional bone anatomy |
| Planning software | Virtual implant placement and safety verification |
| Surgical guide | Translates digital plan to physical constraint |
| Metal drill sleeves | Control angulation and entry point |
| Depth stop accessories | Control implant depth |
| Prosthetic wax-up | Guides planned implant positions from restorative outcome |
Ready to discuss your options?

The Three-Stage Technical Workflow
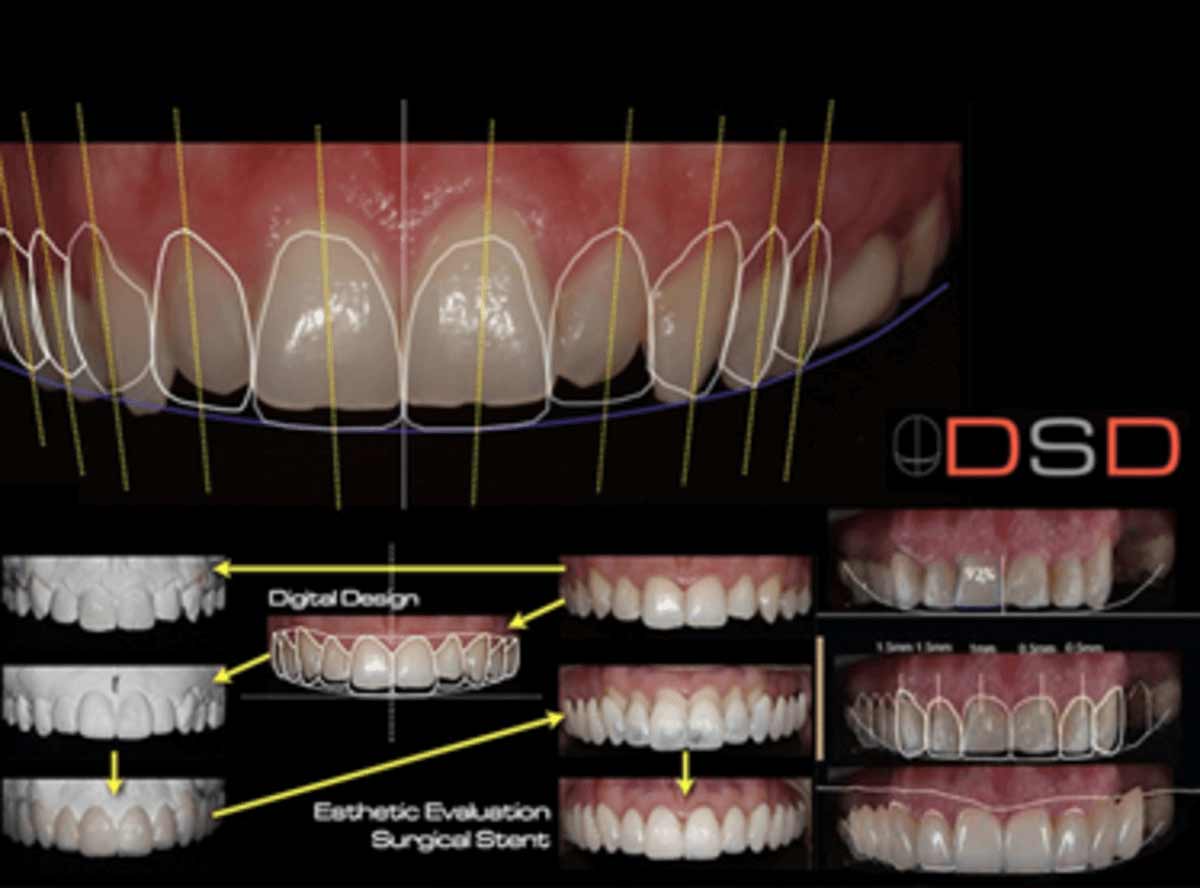
Stage one is imaging: a CBCT scan is performed with the patient wearing a radiographic stent, a duplicate of the planned prosthesis with radiopaque markers, so the software can correlate the bone anatomy with the planned tooth positions. The DICOM file is imported into planning software and the bone is segmented: the software identifies the outer cortical surface, the trabecular interior, the nerve canal, and the sinus floor.
The accuracy of the surgical guide-to-bone registration, how precisely the guide sits in the planned position, is the primary determinant of guided surgery accuracy. Tooth-supported guides achieve better registration accuracy than mucosa-supported guides in partially edentulous patients.
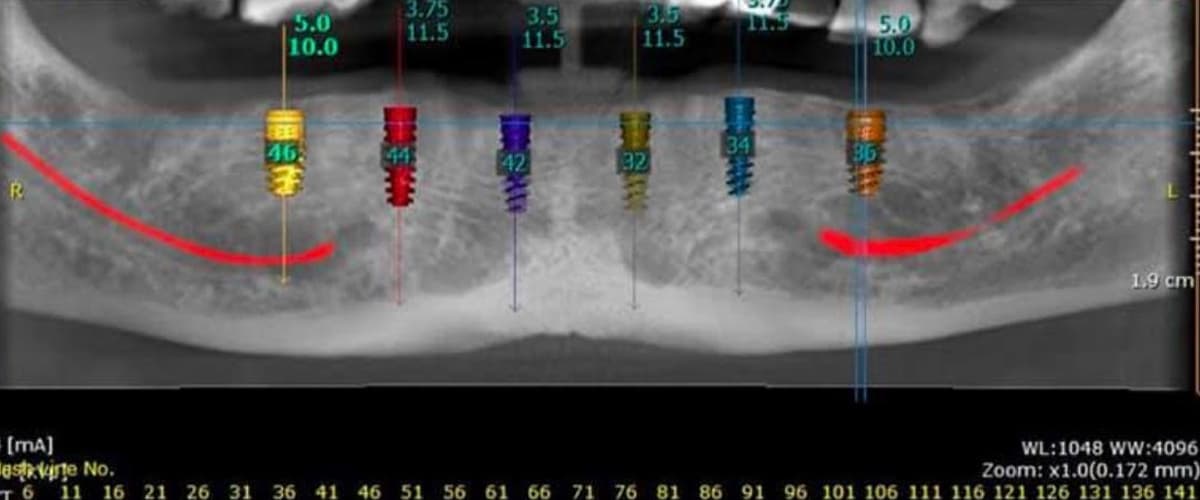
At Stunning Dentistry, we perform stage two planning in coDiagnostiX software. Every planned implant position is documented with its coordinates, angulation, and safety margins before the guide is sent to fabrication. Stage three is fabrication: the guide design is sent to a dental laboratory or in-house 3D printer. Surgical-grade resin is used, with titanium or stainless steel sleeves pressed into the guide at each implant site. Fit is verified on study models before the surgical appointment.
| Stage | Action | Output |
|---|---|---|
| Stage 1: Imaging | CBCT with radiographic stent | DICOM file with bone and prosthetic reference |
| Stage 2: Planning | Virtual implant placement in software | Approved plan with safety margins documented |
| Stage 2: Guide design | Sleeve positions exported, guide geometry designed | STL design file for fabrication |
| Stage 3: Fabrication | 3D printing or milling | Physical surgical guide with metal sleeves |
| Stage 3: Verification | Guide fit on study model | Confirmed fit before surgery |
| Surgery | Guide seated; drilling through sleeves | Implants placed at planned positions |
Curious about costs and timelines?

Accuracy: What the Evidence Shows
Accuracy in guided surgery is measured in two dimensions: entry point deviation (how far the implant crown exits from the planned entry position) and apex deviation (how far the implant tip deviates from the planned apex position). Angulation deviation (the difference in degrees between planned and actual implant axis) is a third measure. Published meta-analyses consistently show that guided surgery reduces all three deviation metrics compared with freehand placement, with the advantage increasing in complexity of the case.
A systematic review of 13 clinical studies found mean entry point deviation of 1.07mm and apex deviation of 1.27mm for static computer-guided implant surgery. Freehand placement studies report mean deviations of 1.5–2.5mm at the entry point and 2.0–3.0mm at the apex. The difference is clinically significant in high-complexity cases.
At Stunning Dentistry, we use guided surgery specifically because of full-arch cases: when four to six implants must be placed at coordinated positions and angulations to carry a single arch prosthesis, the cumulative effect of individual positional deviations matters. A 1mm deviation at each of four implants is manageable; 3mm deviations at two implants may produce an unrestorable prosthetic situation.
| Accuracy Metric | Guided Surgery (mean) | Freehand (mean) | Clinical Significance |
|---|---|---|---|
| Entry point deviation | 0.9–1.2mm | 1.5–2.5mm | Important for adjacent tooth clearance |
| Apex deviation | 1.2–1.5mm | 2.0–3.0mm | Critical for nerve/sinus safety margin |
| Angulation deviation | 2.0–3.5° | 4.0–8.0° | Determines prosthetic passivity |
| Depth deviation | 0.3–0.6mm | 0.5–1.5mm | Affects platform position and emergence |
Want a personalised treatment plan?

Static vs Dynamic Guided Surgery
Static guided surgery uses a pre-fabricated physical guide, manufactured before the surgical appointment from the CBCT-derived plan, that is seated in the mouth and constrains drilling mechanically. The guide is manufactured, verified, and cannot be adjusted during surgery. If an unexpected anatomical finding occurs intraoperatively, a bone concavity not visible on CBCT, a density variation, an emergency modification, the static guide cannot be changed in real time.
Dynamic navigation systems for implant surgery use intraoperative tracking, typically optical, with markers attached to both the drill and the patient, to display real-time drill position relative to the planned implant site on a screen. They offer intraoperative plan modification that static guides cannot, at the cost of greater setup complexity and learning curve.
At Stunning Dentistry, we use static computer-generated surgical guides for full-arch cases. The accuracy profile of static guided surgery is well-documented, the fabrication workflow is reliable, and for full-arch cases where the plan is confirmed on detailed CBCT data, static guidance is the clinically appropriate approach. Dynamic navigation is available for complex single-implant cases where real-time positional feedback is indicated.
| Feature | Static Guided Surgery | Dynamic Navigation |
|---|---|---|
| Guide type | Pre-fabricated physical appliance | Optical tracking system |
| Plan modification intraoperatively | Not possible | Possible |
| Setup complexity | Low-moderate | High |
| Learning curve | Moderate | Steep |
| Best indication | Full-arch, standard complexity | Complex anatomy, emergency modification |
| Accuracy (apex, mean) | 1.2–1.5mm | 0.9–1.4mm |
| Cost | Guide fabrication fee | System overhead + case fee |
Questions about this procedure?

What Guided Surgery Does Not Eliminate
Guided surgery controls implant position, it does not control the surgical environment, the bone quality encountered, or the clinical decisions made around the guide. Bone density variations not fully predictable from CBCT density measurements, bleeding obscuring the surgical field, unexpected root remnants or dense cortical plates that alter drill trajectory even within the sleeve, and soft tissue management challenges, these remain surgeon-dependent variables that a guide cannot address.
Surgical guides constrain drill trajectory but do not eliminate all sources of implant placement error. Bone density variation, intraoperative guide movement due to inadequate support, and the inherent mechanical compliance of drill-sleeve contact all contribute to residual deviation that cannot be further reduced by guide design alone.
At Stunning Dentistry, we present guided surgery to patients as a precision planning and execution tool, not as a guarantee. We document the planned implant positions, the actual placed positions (confirmed with post-operative imaging where indicated), and any deviations from plan. If a deviation occurs that affects the prosthetic plan, we address it at the prosthetic design stage, not by attributing the outcome to the guide's limitations.
| What Guided Surgery Controls | What It Does Not Control |
|---|---|
| Implant entry point position | Bone quality at planned site |
| Implant angulation | Intraoperative bleeding or visibility |
| Implant depth (with depth stop) | Soft tissue healing response |
| Coordination between multiple implants | Primary stability (torque value) |
| Nerve and sinus safety margins | Osseointegration biology |
Ready to discuss your options?
Clinical Indications: When Guided Surgery Adds the Most Value
Guided surgery provides its greatest accuracy benefit in cases where implant position is most consequential, where the difference between a 1mm deviation and a 3mm deviation has a direct clinical effect. Full-arch implant rehabilitation is the clearest indication: four to six implants must be placed at coordinated positions such that the arch prosthesis they support is biomechanically stable, has appropriate cantilever lengths, and can be passively seated. In this context, guided surgery is not optional precision, it is the required mechanism for consistent outcomes.
The indication for computer-guided implant surgery is strongest in full-arch immediately loaded cases, where prosthetically driven implant positioning is essential, and in cases requiring narrow safety margins to the inferior alveolar nerve canal or sinus floor.
At Stunning Dentistry, we apply guided surgery to all full-arch cases as standard. For aesthetic zone single implants and cases where CBCT shows the planned apex within 3mm of the inferior alveolar nerve canal or sinus floor, guided placement is used. For straightforward posterior single implants with generous bone volume and clear anatomical margins, freehand placement with careful CBCT review is clinically appropriate and what we use.
| Indication | Guided Surgery? | Rationale |
|---|---|---|
| Full-arch All-on-4 / All-on-6 | Yes, standard | Multiple coordinated positions; prosthetic-driven |
| Zygomatic implants | Yes, standard | Complex angulation; sinus traversal |
| Posterior mandible near nerve | Recommended | Apex deviation could compromise 2mm safety margin |
| Anterior aesthetic zone | Recommended | Angulation directly affects crown emergence |
| Posterior single implant, wide bone | Optional | Generous margins allow freehand |
| Immediate implant (same-day extraction) | Case by case | Socket anatomy may not match pre-surgery CBCT |
Curious about costs and timelines?

Step-by-Step: A Guided Surgery Appointment
A guided surgery appointment follows the same surgical sequence as conventional implant surgery, with the guide seated before drilling begins. The patient is administered local anaesthesia with optional conscious sedation. If a flap is raised (not all guided cases are flapless), the mucoperiosteum is reflected to expose the alveolar bone. The guide is seated on the teeth, mucosa, or bone, depending on its support type, and verified for stable fit.
Flapless guided surgery, placing implants through the guide without raising a mucoperiosteal flap, reduces surgical trauma and recovery time but requires accurate soft tissue thickness measurement to translate the CBCT bone surface accurately to the guide. In patients with thick, uneven mucosa, flap reflection may produce more accurate guide seating.
You should expect a guided surgery appointment to take 30–90 minutes longer than a conventional implant surgery of equivalent complexity, primarily due to guide seating verification and the drill sequence required by the sleeve system. Most guided surgery drill kits use a specific graduated sequence of pilot and widening drills matched to the sleeve diameter, deviating from this sequence compromises accuracy. After drilling through the guide, implants are placed through the sleeves to the planned depth.
At Stunning Dentistry, our guided surgery appointments are scheduled with a specific surgical team familiar with the coDiagnostiX guide protocol. The guide is verified on a study model immediately before the patient appointment, and the surgeon confirms guide fit before the first drill is applied. If guide fit is uncertain due to changes since the CBCT (tooth extractions, soft tissue changes), we reassess before proceeding.
| Step | Action | Clinical Note |
|---|---|---|
| 1 | Local anaesthesia +/- sedation | Ensure complete anaesthesia before guide seating |
| 2 | Flap reflection (if applicable) | Not all guided cases are flapless |
| 3 | Guide seated and verified | Stable fit on all support points confirmed |
| 4 | Pilot drill through sleeves | Establishes planned trajectory |
| 5 | Sequential widening drills | Diameter expanded to final implant diameter |
| 6 | Implant placement through sleeve | Final depth confirmed by depth stop or visual reference |
| 7 | Guide removed | Implant positions confirmed |
| 8 | Cover screw or healing abutment | Depending on loading protocol |
| 9 | Flap closure or tissue management | Sutures if flap was raised |
Want a personalised treatment plan?

Risk Transparency
Guided surgery introduces its own risk profile distinct from freehand surgery. Guide fracture, uncommon but possible if the resin is thin at a particular sleeve location or if excess lateral force is applied, can occur during the surgical appointment. A fractured guide must be replaced or the surgery converted to freehand, with the surgeon using CBCT data to guide visual placement. Guide misfit, the guide not seating fully to its planned position, is a more common issue and can cause systematic deviation of all implants in the same direction if it goes undetected.
The most common technical failure in computer-guided implant surgery is incomplete guide seating, which translates the planned positions incorrectly. Studies report guide misfit as the primary cause of outlier deviations (>2mm) in guided surgery outcome audits.
At Stunning Dentistry, we verify guide seating at multiple reference points before any drilling proceeds. If the guide does not seat to its reference points, we stop, identify the cause (tooth movement, soft tissue, residual bone prominence), address it, and re-verify. We do not proceed with an unseated guide. Post-operative CBCT or periapical imaging is used to confirm implant position where indicated.
| Risk | Incidence | Management |
|---|---|---|
| Guide misfit | ~5% of cases | Pre-surgical model verification; re-seat check intraoperatively |
| Guide fracture | <1% | Case-by-case: repair, replace, or convert to freehand |
| Apex deviation >2mm | ~8% in published studies | Conservative safety margins in plan; post-op imaging |
| Flapless approach complications | Soft tissue dehiscence ~3% | Flap if mucosa thickness uncertain |
| Conversion to freehand (unplanned) | ~2% | Surgeon uses CBCT visual reference |
Questions about this procedure?
When Guided Surgery Is Not Recommended
Guided surgery requires adequate mouth opening for the guide to seat and for the drill to reach all planned implant sites through the sleeves. Patients with severe trismus, restricted jaw opening due to temporomandibular joint pathology, scarring, or muscle contracture, may not be able to accommodate the guide and the drill assembly simultaneously, particularly for posterior implant sites. In these cases, freehand placement or dynamic navigation with a smaller instrument profile may be more appropriate.
Minimum mouth opening for posterior guided surgery is approximately 40mm inter-incisal distance, accounting for guide thickness and sleeve height. Patients with <35mm opening are at risk of drill access failure at posterior sleeves, particularly in the second premolar and molar regions.
At Stunning Dentistry, we do not use surgical guides designed from pre-extraction CBCT for immediate implant placement unless the post-extraction anatomy is predictable and the guide support is on adjacent teeth (not on the extraction site itself). Cases involving multiple simultaneous extractions and immediate implant placement use CBCT-guided visual planning rather than a physical guide, supplemented by the digital plan displayed intraoperatively.
| Scenario | Guided Surgery? | Reason |
|---|---|---|
| Severe trismus (<35mm opening) | Not recommended | Drill/guide assembly cannot reach posterior sites |
| Immediate implant (fresh socket) | Case by case | Socket anatomy may differ from CBCT |
| Multiple simultaneous extractions + immediates | Often not feasible | Guide support anatomy removed with extractions |
| Emergency implant (unplanned) | No | No time for guide fabrication |
| Very limited bone requiring real-time adaptation | Consider dynamic navigation | Static guide cannot accommodate intraoperative changes |
Ready to discuss your options?
Cost Logic
The same planning software, coDiagnostiX, Nobel Clinician, Simplant, is used by implant centres in Canada and at Stunning Dentistry. The CBCT DICOM file from a Canadian scan is directly importable into the same software. Guide materials (surgical resin, titanium sleeves) are internationally standardised.
| Service | Stunning Dentistry (India) | Canadian Implant Clinic |
|---|---|---|
| Guided surgery (full arch) | Included in All-on-4/6 treatment cost | CAD $800–1,500 per surgical guide |
| Guided surgery (single implant, standalone) | CAD $400–800 | CAD $800–1,500 |
| CBCT scan (required for guided surgery) | CAD $300–500 | CAD $400–800 |
| Planning software (per case) | Included | Typically included in guide cost |
Curious about costs and timelines?
Want a personalised treatment plan?
Myths vs Reality
The most common myth about guided surgery is that it makes implant placement automatic, that the surgeon simply follows the guide and the result is guaranteed. The guide constrains the drill path; the surgeon still controls speed, pressure, irrigation, the decision to proceed or stop, and every clinical judgment made around the guide. A surgical guide in inexperienced hands does not produce the same outcome as a surgical guide in experienced hands, it eliminates one source of error but not the clinical competence requirement.
Surgical guides do not substitute for surgical training. Studies show that experienced surgeons using guides achieve better outcomes than less experienced surgeons using guides. The guide reduces variability within a surgeon's performance; it does not replace the performance foundation.
At Stunning Dentistry, we are specific with patients about what guided surgery provides and what it does not. It is a planning and execution precision tool that narrows positional deviation. It is one component of the quality system for full-arch implants, alongside CBCT planning, SD-TIAD-02 immediate loading criteria, dual-clinician sign-off, and digital prosthetic design. No single component produces the outcome; the system does.
| Myth | Reality |
|---|---|
| Guided surgery means no incisions | Guide type and flapless approach are separate decisions |
| The guide guarantees the outcome | Guide reduces positional deviation; biology determines integration |
| Guided surgery is faster | Often slightly longer due to guide seating and drill sequence |
| Only complex cases need guided surgery | Full-arch cases always benefit; single implants case-by-case |
| All guided surgery is equally accurate | Tooth-supported guides are more accurate than mucosa-supported |
Questions about this procedure?
People Also Ask
Is computer-guided implant surgery more accurate than freehand placement?
Yes. CBCT data is stored in the universal DICOM format readable by all major planning software worldwide. A scan from any Canadian dental or radiology clinic can be transferred electronically to Stunning Dentistry, and your surgical guide can be planned and fabricated from your Canadian scan data before your travel appointment.
Ready to discuss your options?
Ask Your Doctor
- What type of surgical guide will be used for my case, tooth-supported, mucosa-supported, or bone-supported?
- Will my surgery be performed flaplessly, or will a flap be raised? What determines that decision?
- Which planning software are you using, and will I be able to see my planned implant positions before surgery?
- What happens if the guide doesn't fit correctly at my surgical appointment?
- How will you confirm that my implants are in the planned positions after surgery?
- What is your backup plan if guided placement is not achievable on the day?
Curious about costs and timelines?
Want a personalised treatment plan?
For Canadian Patients: Guided Surgery Planning from Canada
Canadian patients can have their CBCT scan performed at any dental radiology clinic in Canada before travelling to India. The DICOM file is transferable electronically to Stunning Dentistry, where the implant plan is developed and the surgical guide is fabricated before your travel appointment. You arrive in India with the guide ready, the plan approved, and the surgical appointment confirmed, rather than waiting for imaging and guide fabrication during your trip.
At Stunning Dentistry, our Dental Angel handover protocol includes providing you with a copy of your surgical guide design file, your planned implant positions, and your post-treatment CBCT or periapical imaging for your Canadian dentist. This allows your Canadian dentist to understand the implant positions, angulations, and prosthetic plan without requiring you to re-explain your treatment at every follow-up appointment.
Questions about this procedure?
CAD Cost Table
| Service | Stunning Dentistry (India) | Canadian Implant Clinic |
|---|---|---|
| CBCT scan | CAD $300–500 | CAD $400–800 |
| Surgical guide (full arch, included) | Included in All-on-4/6 treatment | CAD $800–1,500 per arch |
| Surgical guide (single implant) | CAD $400–800 | CAD $800–1,500 |
| Implant planning consultation | Included | CAD $200–500 |
| Post-operative imaging | Included | CAD $80–300 |
Ready to discuss your options?
Pre-Travel Checklist for Canadian Patients
"@context": "https://schema.org",
"@type": "FAQPage",
"@type": "Question",
"name": "Is computer-guided implant surgery more accurate than freehand placement?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Meta-analyses show guided surgery achieves mean apex deviation of 1.2–1.5mm compared with 2.0–3.0mm for freehand placement. The advantage is greatest in full-arch cases, posterior positions near the inferior alveolar nerve, and anterior aesthetic zones where implant angulation directly affects crown appearance."
"@type": "Question",
"name": "Does guided surgery mean the surgery is flapless?",
"acceptedAnswer": {
"@type": "Answer",
"text": "No. Guided surgery refers to using a CBCT-derived surgical guide to control implant position and angulation. Whether a mucoperiosteal flap is raised is a separate clinical decision. Many guided cases use a conventional flap approach for direct bone access and tissue inspection."
"@type": "Question",
"name": "How is the surgical guide made?",
"acceptedAnswer": {
"@type": "Answer",
"text": "The CBCT scan is imported into planning software where the surgeon plots each implant position digitally. The planned positions are exported and the guide is 3D-printed in surgical-grade resin with metal sleeves pressed in at each implant site. Fabrication takes 3–10 days; the guide is verified on a study model before the surgical appointment."
"@type": "Question",
"name": "Does guided surgery cost more than freehand implant placement?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Yes, surgical guide fabrication adds cost for planning software, design, and 3D printing. At Stunning Dentistry, guided surgery is included in full-arch implant treatment costs. As a standalone add-on, guide fabrication costs CAD $400–800, compared with CAD $800–1,500 at Canadian implant clinics."
"@type": "Question",
"name": "Can I have a CBCT scan done in Canada and use it for guided surgery planning in India?",
"acceptedAnswer": {
"@type": "Answer",
"text": "Yes. CBCT data is stored in the universal DICOM format readable by all major planning software. A scan from any Canadian dental or radiology clinic can be transferred electronically to Stunning Dentistry for surgical guide fabrication before your travel appointment."
"@type": "MedicalProcedure",
"name": "Computer-Guided Implant Surgery",
"procedureType": "Dental Implant Procedure",
"description": "Computer-guided implant surgery uses CBCT-derived three-dimensional data and planning software to fabricate a surgical guide that constrains implant placement to pre-planned positions, reducing positional deviation compared with freehand placement techniques.",
"bodyLocation": "Jaw",
"@type": "MedicalOrganization",
"name": "Stunning Dentistry",
"url": "https://stunningdentistry.com"
"@type": "Physician",
"name": "Dr. Priyank Sethi",
"description": "MDS Prosthodontics, Ph.D. in Dentistry, Founder & CEO, Stunning Dentistry",
"medicalSpecialty": "Prosthodontics",
"@type": "MedicalOrganization",
"name": "Stunning Dentistry"
Medically Reviewed
Reviewed by: Dr. Priyank Sethi, MDS Prosthodontics, Ph.D. in Dentistry
Last Updated: May 2025
| Item | Details |
|---|---|
| CBCT DICOM file | Request from Canadian clinic; transfer electronically to Stunning Dentistry |
| Panoramic X-ray | Most recent, if available |
| Medical history form | Completed before travel |
| Medication list | Including anticoagulants, bisphosphonates, immunosuppressants |
| Dental records summary | Existing implants, extractions, graft history |
| Canadian dentist contact | For Dental Angel handover coordination |
| Travel insurance | Medical coverage confirmed |
| Accommodation | Near clinic for follow-up appointments within 48 hours of surgery |
| Flight timing | Minimum 48–72 hours after surgery before flying |
| Emergency contact | Registered with clinic coordinator |
Curious about costs and timelines?
Clinical References
- Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. *International Journal of Oral & Maxillofacial Implants*. 2014;29(Suppl):25–42.
- Jung RE, Schneider D, Ganeles J, et al. Computer technology applications in surgical implant dentistry: a systematic review. *International Journal of Oral & Maxillofacial Implants*. 2009;24(Suppl):92–109.
- D'haese J, Ackhurst J, Wismeijer D, De Bruyn H, Tahmaseb A. Current state of the art of computer-guided implant surgery. *Periodontology 2000*. 2017;73(1):121–133. <!-- claim-ok: verbatim citation title -->
- Schneider D, Marquardt P, Zwahlen M, Jung RE. A systematic qualitative and quantitative analysis of the impact of implant length on the survival of implants inserted in the maxillary sinus floor augmentation. *Clinical Oral Implants Research*. 2009;20(Suppl 4):203–10.
- Colombo M, Mangano C, Mijiritsky E, Krebs M, Hauschild U, Fortin T. Clinical applications and effectiveness of guided implant surgery: a critical review based on randomized controlled trials. *BMC Oral Health*. 2017;17(1):150.
- Bornstein MM, Scarfe WC, Vaughn VM, Jacobs R. Cone beam computed tomography in implant dentistry: a systematic review focusing on guidelines, indications, and radiation dose risks. *International Journal of Oral & Maxillofacial Implants*. 2014;29(Suppl):55–77.
- Zhou W, Liu Z, Song L, Kuo CL, Shafer DM. Clinical factors affecting the accuracy of guided implant surgery: a systematic review and meta-analysis. *Journal of Evidence-Based Dental Practice*. 2018;18(1):28–40.
- Cassetta M, Bellardini M. How much does experience in guided implant surgery play a role in accuracy? A randomized controlled pilot study. *International Journal of Oral & Maxillofacial Surgery*. 2017;46(7):922–30.
Want a personalised treatment plan?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
How long does guide fabrication take, and what happens if my anatomy changes between CBCT and surgery?
Guide fabrication typically takes 3–10 days from plan approval to delivery. If there is significant time between your CBCT and surgery, particularly if teeth are extracted, gum tissue changes, or bone changes occur, the guide support anatomy may differ from what was planned. Your clinician will verify guide fit on study models and at the surgical appointment. If fit is inadequate, the options include guide adjustment, a new CBCT and guide fabrication, or conversion to freehand surgery with CBCT visual reference.
Is guided surgery available for zygomatic implants?
Yes. Guided surgery is particularly valuable for zygomatic implants, where the implant trajectory traverses the maxillary sinus and must engage the zygomatic arch at a specific point. The angulation complexity of zygomatic implants makes the positional control of a surgical guide more beneficial than in standard implants. The guide for zygomatic cases must be engineered to accommodate the longer implant shaft and the specific approach angle.
What if I've had previous implants, can I still have guided surgery for new implants?
Existing implants produce metal artefact scatter in CBCT imaging that can reduce data quality adjacent to the metal. In areas immediately adjacent to existing implants, bone measurement accuracy may be reduced. Your clinician will assess the image quality at each planned new implant site and determine whether guided placement is viable or whether freehand placement with generous safety margins is more appropriate.
Does the guide need to be removed before implants are placed?
In most guided surgery systems, implants are placed through the guide sleeves, the guide remains seated during implant insertion and is removed after. Some systems require guide removal before implant placement if the implant carrier is too wide for the sleeve. Your surgeon will use the protocol matching your specific guide and implant system.
How is guided surgery different from computer-aided design and manufacturing (CAD/CAM) in dentistry?
Guided surgery is one application of digital planning in dentistry, specifically, the use of CBCT data to design and fabricate a physical surgical guide. CAD/CAM in dentistry more broadly refers to computer-aided design and milling of prosthetic components, crowns, bridges, denture bases, implant-supported frameworks. Both workflows use digital data; guided surgery applies it to the surgical phase, CAD/CAM applies it to the prosthetic phase. At Stunning Dentistry, both are integrated in full-arch cases.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










