All-on-4 Dental ImplantsFixed Full-Arch Teeth on Four Implants, Without Bone Grafting
- All-on-4 exists because conventional implant dentistry frequently demands more bone than edentulous patients have left.
When bone loss makes four vertical implants impossible, placing two of those implants at a posterior tilt of 30–45 degrees changes the geometry, distributing occlusal force across a longer lever arm, reaching denser anterior bone, and eliminating the grafting requirement entirely.
Overview
All-on-4 exists because conventional implant dentistry frequently demands more bone than edentulous patients have left. When bone loss makes four vertical implants impossible, placing two of those implants at a posterior tilt of 30–45 degrees changes the geometry, distributing occlusal force across a longer lever arm, reaching denser anterior bone, and eliminating the grafting requirement entirely. The result is a full-arch fixed prosthesis on four fixtures that integrates without augmentation.
The tilted-implant concept was not a compromise for poor bone, it was a biomechanical redesign that outperforms the vertical four-implant model in specific anatomical conditions.
At Stunning Dentistry, All-on-4 is executed under the SD-FMR-05 protocol: dual-clinician sign-off before any irreversible surgical step, CBCT-guided planning with Nobel Clinician or coDiagnostiX software, and Straumann, Nobel Biocare, or Osstem fixture systems with documented 10-year survival data.
Questions about this procedure?
What Is All-on-4?
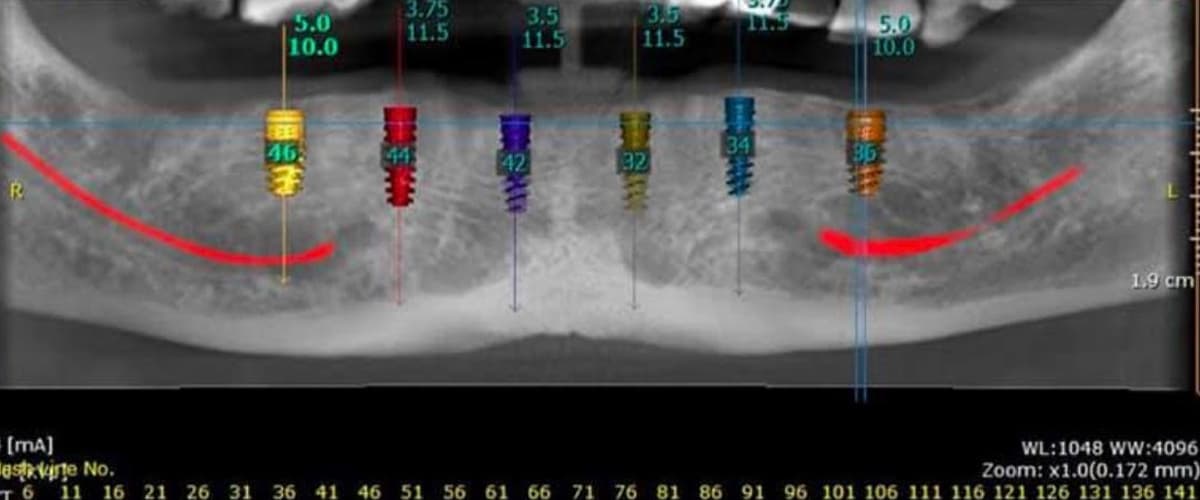
All-on-4 is a full-arch implant reconstruction protocol in which a complete dental arch, typically 10–14 teeth, is supported by exactly four endosseous implants. Two implants are placed vertically in the anterior jaw. Two are placed at a 30–45-degree posterior tilt, engaging denser cortical bone further from the alveolar ridge and extending the prosthetic anchorage base without grafting.
Ten-year implant survival rates for All-on-4 range from 94.8% to 98.0% in published multi-centre trials, with prosthetic survival rates of 93.7% to 99.5%.
At Stunning Dentistry, we explain the All-on-4 biomechanical design in your CBCT analysis appointment before you make any decisions. Patients who understand the mechanism, not just the outcome, make better treatment decisions and follow aftercare protocols more accurately.
Ready to discuss your options?

Why Tilted Implants Work
The sinus floor and the mental foramen constrain conventional vertical implant placement in the posterior jaw. Tilted implants bypass both: the posterior pair engages bone anterior to the sinus in the maxilla and anterior to the mental foramen in the mandible, bone that is consistently denser and more available in severely resorbed arches.
Posterior tilting of 30–45 degrees increases the A-P spread by 6–10 mm compared with four parallel vertical fixtures in the same arch, reducing cantilever length and peak crestal bone stress.
At Stunning Dentistry, we use coDiagnostiX software to plan all posterior tilt angles against your specific CBCT anatomy before surgery begins. The tilt is not estimated, it is calculated from your bone geometry.
Curious about costs and timelines?
Long-Term Survival Data
Mandible survival rates consistently exceed maxillary rates. The difference reflects cortical bone density: mandibular bone is denser, primary stability is more reliable, and osseointegration proceeds under better mechanical conditions. Both arches produce clinically acceptable outcomes when patient selection is protocol-driven.
| Study / Source | Follow-Up | Implant Survival | Prosthesis Survival | Notes |
|---|---|---|---|---|
| Malo et al. (2019) | 10 years | 94.8% mandible | 99.5% | Multi-centre, 245 patients |
| Malo et al. (2019) | 10 years | 95.6% maxilla | 93.7% | Immediate loading subgroup |
| Soto-Penaloza et al. (2017) | Systematic review | 98.0% | 99.2% | 19 studies, 1,285 patients |
| Francetti et al. (2015) | 5 years | 97.5% | 98.1% | 242 patients, 3 centres |
| Babbush et al. (2014) | 3 years | 98.7% | 100% | Immediate-load cohort |
Want a personalised treatment plan?
Who Is a Candidate?
All-on-4 candidacy is determined by bone quantity, bone quality, systemic health, and occlusal load requirements, not age, not tooth count alone. A 45-year-old with advanced periodontitis and insufficient bone may be a stronger All-on-4 candidate than a 70-year-old with a single failing arch.
Uncontrolled diabetes (HbA1c ≥8.0%), active bisphosphonate use with BRONJ history, and heavy unmanaged bruxism represent relative contraindications requiring specialist review before proceeding.
At Stunning Dentistry, every All-on-4 consultation includes CBCT analysis, ISQ planning, and a systemic health screen before we discuss surgical scheduling. No irreversible step is taken until candidacy is confirmed in writing under the SD-FMR-05 protocol.
Questions about this procedure?
Graftless Protocol
The primary reason patients choose All-on-4 over conventional full-arch implant rehabilitation is the elimination of bone grafting. Grafting adds 4–9 months of healing time, a second surgical site and its associated morbidity, additional cost (CAD $3,000–$8,000 per site), and a period of functional compromise during graft maturation. All-on-4's tilted implant design avoids all of this by reaching bone that is already there.
Graftless All-on-4 protocols demonstrated equivalent or superior long-term outcomes compared with grafted conventional implant placements in matched cohort studies, with substantially reduced morbidity and treatment time.
At Stunning Dentistry, our graftless protocol applies to All-on-4, All-on-6, and zygomatic implant cases. The decision tree is anatomy-driven: your CBCT determines which graftless path, if any, your bone geometry supports.
Ready to discuss your options?

Immediate Loading
Immediate loading, placing a functional prosthesis on the day of surgery, is achievable in most All-on-4 cases when primary stability meets the clinical threshold. The provisional prosthesis is load-protected: it is designed for soft-tissue contact, not molar occlusal force, and the patient follows a soft diet for 8–12 weeks while osseointegration completes.
Immediately loaded All-on-4 implants achieved equivalent osseointegration rates to delayed-load controls at 12 months, with no statistically significant difference in marginal bone loss.
At Stunning Dentistry, immediate loading is gated under our SD-TIAD-02 protocol: insertion torque ≥35 Ncm at each implant, ISQ ≥60 confirmed with the Osstell Beacon, cross-arch splinting, and bruxism/parafunction screening before the provisional is placed. If any gate fails intra-operatively, we stage to delayed loading. Teeth on the same day is a clinical outcome, not a marketing promise.
Curious about costs and timelines?

Benefits
All-on-4 delivers fixed, non-removable teeth in one surgical appointment with no bone grafting in most cases, no removable denture transition in qualifying patients, and a 4–6 month total timeline to the definitive zirconia or hybrid prosthesis. The functional benefits begin the same day: chewing force returns to approximately 80% of natural dentition within 12 weeks as osseointegration matures.
Oral health-related quality of life (OHRQoL) scores improved by a mean of 42 points on the OHIP-14 scale at 12 months following immediately loaded All-on-4, with satisfaction scores exceeding 90% across eating, speech, and appearance domains.
At Stunning Dentistry, every All-on-4 case documents baseline OHRQoL, bite force, and clinical photography before treatment and at 12-month review. Outcomes are tracked against protocol, not described in marketing language.
Want a personalised treatment plan?

Recovery Timeline
| Phase | Timeframe | What Happens | Your Responsibility |
|---|---|---|---|
| Surgical Day | Day 0 | Implant placement, provisional fixed in mouth | Accompanied transport, do not drive |
| Acute Healing | Days 1–7 | Swelling peaks Day 2–3, soft diet, prescribed rinse | Ice 20 min on/off, liquid to soft diet, no straws |
| Early Integration | Weeks 2–8 | Osseointegration progresses, provisional functioning | Soft diet maintained, no hard/crunchy foods |
| Provisional Review | Week 8–10 | ISQ re-measured, occlusion checked, impressions if stable | Attend review, report any implant movement |
| Definitive Impressions | Months 3–4 | Final digital or physical impressions for zirconia prosthesis | Attend all impressions and try-in appointments |
| Definitive Fit | Months 4–6 | Definitive monolithic zirconia or hybrid prosthesis fitted | Attend fit appointment, follow torque protocol |
| 12-Month Review | Month 12 | Periapical X-rays, marginal bone level measured, ISQ checked | Attend review, maintain cleaning protocol |
Questions about this procedure?
Complications
Complications in All-on-4 fall into two categories: biological (implant-related) and mechanical (prosthesis-related). Biological complications include peri-implantitis (cumulative 5-year incidence ~8–12%), implant fracture (<1%), and sinusitis in maxillary cases involving proximity to the sinus floor. Mechanical complications include abutment screw loosening (most common, managed with re-torquing), prosthesis fracture in hybrid PMMA provisionals, and occlusal wear of the definitive prosthesis over 8–12 years.
Peri-implantitis was the most common biological complication in 10-year All-on-4 follow-up, with a cumulative incidence of 9.7%, predominantly in patients with a history of periodontitis and poor oral hygiene compliance.
At Stunning Dentistry, complications are discussed in your pre-surgical informed consent documentation, not mentioned only when they occur. You receive a written aftercare protocol before surgery, a emergency contact number with a documented response commitment, and a network of partner-friendly dentists in Canada for your local follow-up.
Ready to discuss your options?
Comparison Table
| Factor | All-on-4 | All-on-6 | Zygomatic | Overdenture (2-implant) |
|---|---|---|---|---|
| Implant Count | 4 | 6 | 2–4 zygomatic + 0–4 standard | 2–4 |
| Bone Requirement | Moderate anterior | Moderate | Severe atrophy (no posterior) | Low |
| Bone Grafting | None (usually) | None (usually) | None | None |
| Cantilever | Reduced | Minimal or none | None | N/A (removable) |
| Immediate Loading | Yes (gated) | Yes (gated) | Yes (gated) | Yes |
| Prosthesis Type | Fixed | Fixed | Fixed | Removable (snap-on) |
| Timeline to Definitive | 4–6 months | 4–6 months | 4–6 months | 2–3 months |
| CAD Cost (Stunning Dentistry) | $14,000–$20,000 per arch | $16,000–$24,000 per arch | $22,000–$32,000 per arch | $8,000–$12,000 per arch |
| CAD Cost (Canada private) | $45,000–$65,000 | $55,000–$75,000 | $70,000–$100,000 | $20,000–$35,000 |
Curious about costs and timelines?
Cost Factors
All-on-4 cost is determined by five variables: implant system (Straumann SLActive vs Nobel Biocare Active vs Osstem TSIII), prosthesis material (monolithic zirconia vs hybrid metal-acrylic vs PMMA provisional), arch count (single vs dual arch), sedation modality (local + oral sedation vs IV sedation vs general anaesthesia), and ancillary procedures (extractions, bone contouring, sinus management).
Canadian public system: Not available for elective implant treatment
| Cost Factor | Lower Range | Higher Range | Driver |
|---|---|---|---|
| Implant system | Osstem TSIII | Straumann SLActive | Surface technology, survival data tier |
| Prosthesis material | PMMA hybrid | Monolithic 5Y-TZP zirconia | Material cost, milling time, lab fees |
| Arch count | Single arch | Dual arch (upper + lower) | Volume of surgery and prosthetics |
| Sedation | Oral + local | IV or GA | Anaesthetic fee, monitoring |
| Extractions | None remaining | Multiple surgical extractions | Number and complexity |
Want a personalised treatment plan?

Step-by-Step
Day 1, CBCT Imaging and Treatment Planning: Your cone-beam CT scan is acquired and analysed in Nobel Clinician or coDiagnostiX software. The implant positions, depths, and angles are planned digitally against your bone anatomy. The surgical guide is designed from this plan.
Day 2–3, Extraction and Site Preparation (if required): Remaining teeth requiring extraction are removed in the same appointment as or immediately preceding implant placement. Alveolar bone is contoured where required for prosthetic fit.
Day 3–4, Implant Surgery: Under local anaesthesia with sedation available, the four implants are placed per the surgical guide plan. Insertion torque is measured at each implant. If all four meet the ≥35 Ncm threshold and ISQ ≥60, the provisional prosthesis is prepared.
Day 4, Provisional Fitting: The provisional prosthesis, pre-fabricated or chairside-milled, is adjusted for occlusion, fitted to the implant abutments, and fixed with prosthetic screws. Occlusal contacts are reduced on the provisional to protect primary stability.
Week 8–10, Review and Stability Confirmation: ISQ is re-measured. Occlusion and soft tissue are assessed. Digital or conventional impressions are taken for the definitive prosthesis if integration is confirmed.
Month 4–6, Definitive Prosthesis Delivery: The definitive monolithic zirconia or hybrid prosthesis is fitted, occlusion is finalised, and torque values are recorded. The patient receives their written aftercare protocol and emergency contact information.
Questions about this procedure?
Aftercare
Aftercare for All-on-4 is a clinical protocol, not a suggestion. The prosthesis is fixed and cannot be removed for cleaning, the maintenance strategy is access-based: interdental brushes (size 1.0–1.5 mm for the implant-gingival interface), water flosser at medium pressure (not jet), and a soft-headed electric toothbrush for the prosthetic surfaces.
Patients who maintained a ≥6-monthly professional cleaning protocol showed marginal bone loss of 0.8 mm at 5 years. Non-compliant patients showed 2.1 mm, a statistically and clinically significant difference.
At Stunning Dentistry, you receive a written aftercare protocol at definitive delivery. Your Canadian home dentist receives a clinical handover document specifying implant specifications, torque values, prosthesis materials, and the cleaning protocol. This documentation is part of the Dental Angel service, not an optional add-on.
Ready to discuss your options?
Aftercare Responsibility Split
| Task | Frequency | Who | How |
|---|---|---|---|
| Daily brushing of prosthesis surfaces | Twice daily | Patient | Soft electric toothbrush |
| Interdental brush under prosthesis | Daily | Patient | Size 1.0–1.5 mm Curaprox or TePe |
| Water flosser irrigation | Daily | Patient | Medium pressure, 45° angle at gingival margin |
| Professional ultrasonic cleaning | Every 6 months | Home dentist | Subgingival access around each abutment |
| Periapical X-ray for bone levels | Annually | Home dentist | 4 periapical films at implant sites |
| Occlusal check and screw torque | Annually | Home dentist or Stunning Dentistry | Torque driver to 15–25 Ncm per abutment |
| Prosthesis removal and deep clean | Every 3–5 years | Stunning Dentistry or referred prosthodontist | Full removal, clean, re-insertion |
Curious about costs and timelines?
When All-on-4 Is Not Recommended
All-on-4 is contraindicated when the anatomical or systemic conditions that make it effective, anterior bone volume, achievable primary stability, and manageable parafunction, cannot be confirmed. The procedure's biomechanical logic depends on tilted posterior implants and a specific anterior-posterior spread; if the bone geometry cannot support that arrangement, the risk profile changes materially.
Absolute contraindications to full-arch immediate implant rehabilitation include uncontrolled systemic disease affecting bone metabolism, active local infection, and insufficient bone volume for the planned implant count without augmentation. Relative contraindications require case-by-case risk assessment.
At Stunning Dentistry, we document contraindications explicitly in the treatment planning record before any surgical scheduling. If All-on-4 is not the right architecture for your anatomy or systemic status, we explain the alternative, All-on-6, zygomatic implants, or staged rehabilitation, and the clinical rationale for the recommendation in writing.
| Contraindication | Type | Path Forward |
|---|---|---|
| Insufficient anterior bone (no grafting plan) | Absolute | Zygomatic implants or phased bone graft |
| Uncontrolled diabetes (HbA1c >9%) | Absolute until stabilised | Defer; re-evaluate at HbA1c ≤7% |
| Active oral or systemic infection | Absolute until resolved | Treat infection, 6-week wait, re-plan |
| Heavy unmanaged bruxism | Relative | Night splint protocol + delayed loading |
| IV bisphosphonate therapy | Absolute | Oncology/prescriber consultation required |
| Oral bisphosphonate, low-dose, short-term | Relative | Risk stratification with prescriber |
| Intra-operative gate failure (SD-TIAD-02) | Converts to staged protocol | Delayed loading at 8–12 weeks |
Want a personalised treatment plan?

Myths vs Reality
"Four implants aren't enough to hold a full arch."
At 10 years, multi-centre All-on-4 data shows implant failure rates of 2–5.2%. This is lower than the 5-year failure rate for single crowns on root-treated teeth and significantly lower than the failure rate of complete dentures in terms of functional adequacy.
Questions about this procedure?
People Also Ask
How long do All-on-4 implants last in Canada?
All-on-4 implant systems carry published 10-year survival data of 94.8–98.0% at the implant level and 93.7–99.5% at the prosthetic level in multi-centre trials.
The prosthesis typically requires replacement or refinishing at 10–15 years depending on the material, monolithic zirconia lasts longer than hybrid acrylic. Implant survival continues beyond prosthetic lifespan in most cases.
All-on-4 surgery is performed under local anaesthesia with sedation options available for patients who require it.
The procedure itself produces pressure sensation, not pain. Post-operative discomfort is managed with prescription analgesics for the first 3–5 days; most patients describe it as comparable to a complex tooth extraction.
The provisional prosthesis requires a soft diet for 8–12 weeks while osseointegration completes.
After the definitive zirconia prosthesis is placed at 4–6 months, masticatory function is approximately 80% of natural dentition, adequate for the full range of normal foods with the exception of very hard items (ice, hard candy, bones).
Private prosthodontic fees for All-on-4 in Canadian cities range from CAD $45,000–$65,000 per arch.
Public dental coverage does not include implant-based prosthetics. Stunning Dentistry's all-inclusive fee is CAD $14,000–$20,000 per arch, performed in India with the same implant systems used in Canadian clinics.
What is the difference between All-on-4 and All-on-6?
All-on-4 uses four implants with posterior tilt to maximise A-P spread; All-on-6 uses six implants with reduced or no distal cantilever.
All-on-6 is indicated for larger arches, heavier bite forces, monolithic zirconia restorations requiring maximum support, and cases where cantilever reduction is the clinical priority.
Ready to discuss your options?
Ask Your Doctor
1. What is my measured A-P spread on CBCT and does it support a full-arch prosthesis on four implants without cantilever risk?
2. What are the planned tilt angles for my posterior implants and which bone layer are they engaging?
3. What insertion torque and ISQ thresholds do you use as the gate for same-day loading?
4. If same-day loading is not achievable on the day, what is the staged alternative?
5. Which implant system do you use and what is its published 10-year survival data?
6. What prosthesis material will my provisional be, and what is my definitive prosthesis plan?
7. What is the written warranty on the implants and the prosthesis?
8. What is the protocol if I develop peri-implantitis after I return to Canada?
9. How will my Canadian dentist be briefed on my case, and what documentation will they receive?
10. What does the aftercare protocol require of me, and what happens if I miss a cleaning appointment?
Curious about costs and timelines?
For Canadian Patients
Canadian patients considering All-on-4 face a specific structural problem: the Canadian prosthodontic system charges CAD $45,000–$65,000 per arch for implant-based full-arch reconstruction, provincial insurance does not cover implant prosthetics, and wait times for specialist consultation in major cities run 3–6 months before surgery is even scheduled. Patients in smaller provinces face additional barriers: no local prosthodontist, referral to a distant city, and the same high fee without reduced travel cost.
Dental implant coverage in Canada remains limited to provincial assistance programs for low-income individuals, with implant-based prosthetics generally excluded. Private insurance coverage for full-arch implant cases is rarely available.
At Stunning Dentistry, Canadian patients receive the Dental Angel service: pre-departure consultation, airport transfer, accommodation coordination, daily clinical check-in during the surgical week, and a written clinical handover for their Canadian dentist. The handover document includes implant specifications, torque values, prosthesis materials, and the full aftercare protocol, so your home dentist has everything they need for your annual review.
Want a personalised treatment plan?
CAD Cost Table
| Item | Stunning Dentistry (CAD) | Canadian Private Clinic (CAD) | Difference |
|---|---|---|---|
| All-on-4 single arch (implants + provisional) | $10,000–$14,000 | $35,000–$50,000 | ~$25,000–$36,000 |
| Definitive zirconia prosthesis (per arch) | $4,000–$6,000 | $10,000–$15,000 | ~$6,000–$9,000 |
| CBCT imaging | Included | $500–$1,200 | Included |
| Surgical guide | Included | $1,000–$2,000 | Included |
| Sedation (IV) | $500–$800 | $1,500–$3,000 | ~$1,000–$2,200 |
| Return flights (Toronto–India economy) | $1,200–$1,800 | N/A | N/A |
| Accommodation (10–14 nights) | $800–$1,400 | N/A | N/A |
| **Total (single arch, complete)** | **~$14,000–$20,000** | **~$45,000–$65,000** | **~$31,000–$45,000** |
Questions about this procedure?
Decision Framework
| Question | If Yes | If No |
|---|---|---|
| Is the Canadian fee within your budget without compromising your financial position? | Consider Canadian clinic | Evaluate Stunning Dentistry |
| Do you have a complex medical history requiring in-country specialist oversight? | Consult local oral surgeon first | Proceed with evaluation |
| Is your bone anatomy confirmed as All-on-4 compatible by CBCT? | All-on-4 is indicated | Evaluate All-on-6 or zygomatic |
| Are you prepared to travel for two trips (10–14 days + 5–7 days)? | Yes, proceed | Consider delayed single-trip protocol |
| Do you have a Canadian dentist willing to follow the handover protocol? | Proceed | Dental Angel service identifies a local provider |
Ready to discuss your options?
Pre-Travel Checklist
| Item | Status |
|---|---|
| CBCT scan from a Canadian dental clinic (if available), sent in advance | ☐ |
| Full medical history form completed and submitted to Stunning Dentistry | ☐ |
| Medications list including bisphosphonates, blood thinners, diabetes medications | ☐ |
| Canadian dentist briefed on planned treatment and willing to receive handover | ☐ |
| Return flights booked: minimum 10 days for surgical trip, 5 days for definitive | ☐ |
| Accommodation arranged (Stunning Dentistry Dental Angel can coordinate) | ☐ |
| Travel insurance covering dental complications confirmed | ☐ |
| Soft food provisions planned for post-surgical week | ☐ |
| Emergency contact number for Stunning Dentistry saved | ☐ |
Curious about costs and timelines?
Want a personalised treatment plan?
Clinical References
1. Malo P, de Araujo Nobre M, Lopes A, et al. All-on-4 treatment concept for the rehabilitation of the completely edentulous mandible: A 7-year clinical and 5-year radiographic retrospective case series. *Clin Implant Dent Relat Res.* 2019.
"name": "Stunning Dentistry"
Questions about this procedure?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
Do I need to remove my All-on-4 prosthesis to clean it?
No, the prosthesis is fixed with prosthetic screws and is not removed by the patient. Daily cleaning is performed in-mouth using an interdental brush (1.0–1.5 mm) and water flosser. Professional removal for deep cleaning is recommended every 3–5 years.
What happens if one of the four implants fails?
Single implant failure in a four-implant arch requires assessment of the prosthesis loading distribution. In many cases, the arch can be maintained on three implants temporarily while the failed site is evaluated for re-implantation. All-on-6 provides an additional implant as redundancy, a consideration in high-risk patients.
Can I have All-on-4 if I have been told I have too little bone?
CBCT imaging is required to determine whether your anterior bone supports the All-on-4 graftless protocol. Many patients referred for grafting before conventional implants are in fact All-on-4 candidates. Some are zygomatic implant candidates. The evaluation determines your path.
How many trips to India does All-on-4 require?
Most patients complete All-on-4 in one trip of 10–14 days covering pre-surgical imaging, surgery, provisional fitting, and initial healing review. The definitive prosthesis fitting requires a second trip at 4–6 months, typically 5–7 days. ---
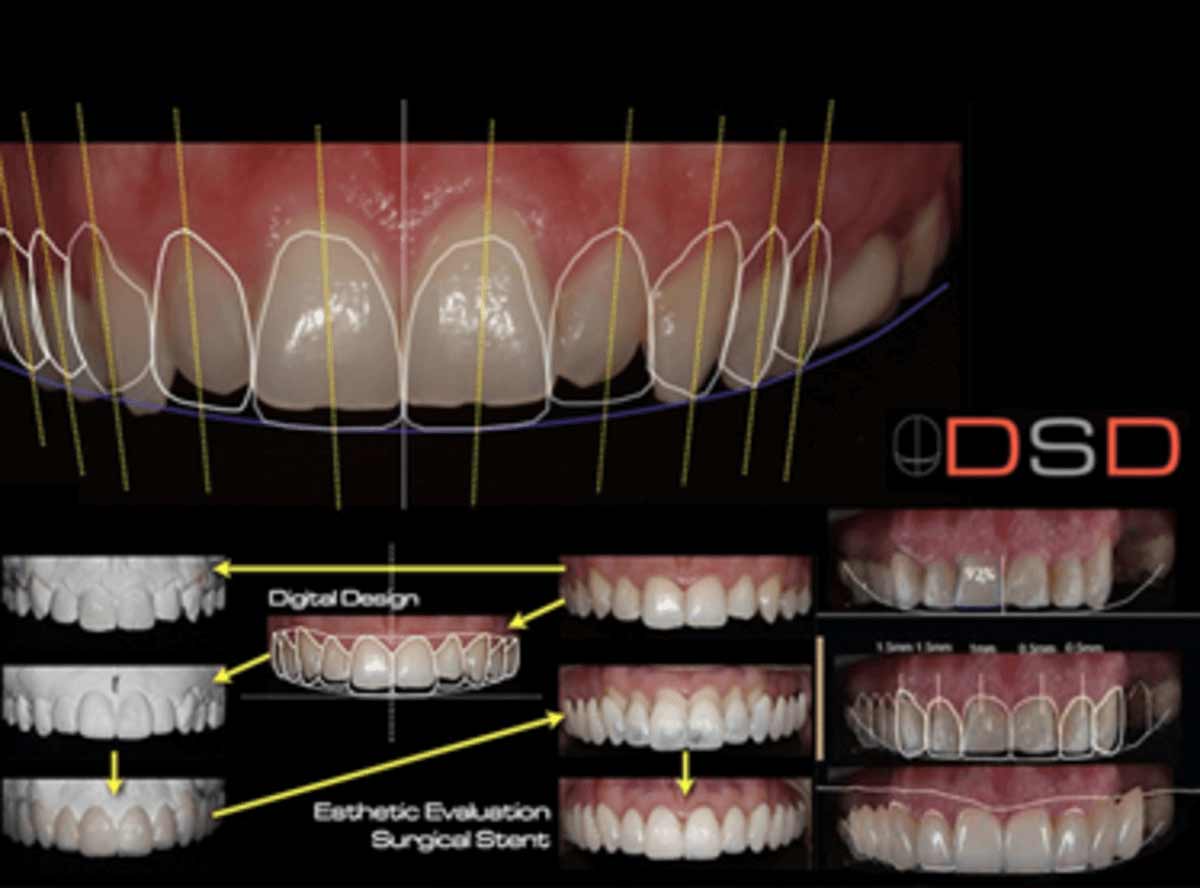
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










