Smile Design in CanadaDigital Planning, Aesthetic Protocols, and What the Process Actually Involves
- Smile design is not a single dental procedure, it is a planning and execution framework that coordinates multiple aesthetic and restorative treatments to achieve a defined outcome.
The distinguishing characteristic of a structured smile design approach, versus unsystematic cosmetic treatment, is the sequence: aesthetic analysis and digital planning precede any irreversible preparation of teeth.
Overview
What is smile design, and what does the process involve?
> Smile design is a structured treatment planning methodology that uses digital imaging, facial proportion analysis, and clinical assessment to create a predictable aesthetic treatment plan before any irreversible dentistry begins. It typically incorporates dental veneers, crowns, composite bonding, tooth whitening, and gum contouring, selected and sequenced to achieve a specific visual and functional outcome planned in advance through digital mock-up.
Smile design is not a single dental procedure, it is a planning and execution framework that coordinates multiple aesthetic and restorative treatments to achieve a defined outcome. The distinguishing characteristic of a structured smile design approach, versus unsystematic cosmetic treatment, is the sequence: aesthetic analysis and digital planning precede any irreversible preparation of teeth. The patient sees and approves a digital simulation and a temporary mock-up in their own mouth before the permanent restorations are prepared and delivered.
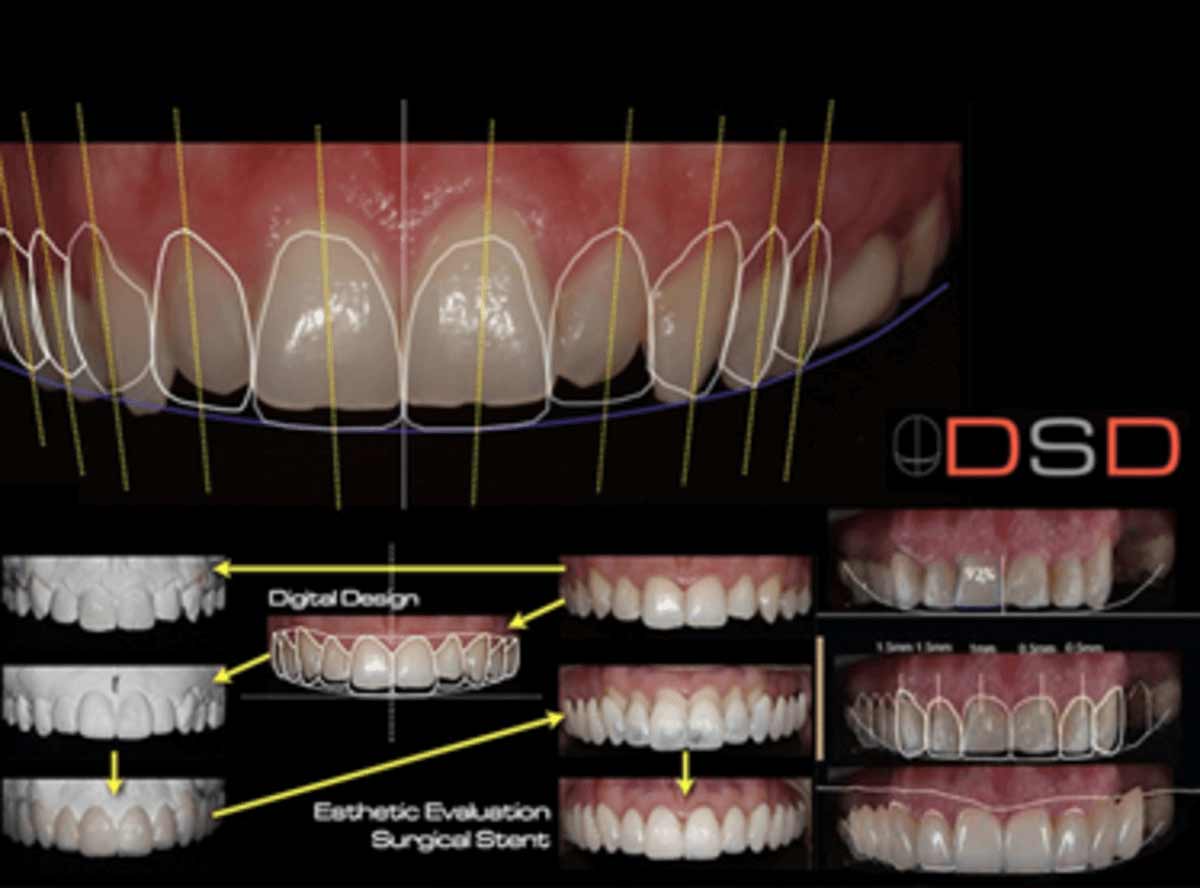
At Stunning Dentistry, we begin all smile design cases with a full facial and dental digital analysis, photographs, digital smile design (DSD) software mapping, and a diagnostic wax-up, before any treatment plan is presented. Patients see a digital preview and a physical mock-up that they can try in their mouths before the final plan is approved. No irreversible tooth preparation takes place until the patient has confirmed the planned outcome in the mock-up phase.
| Approach | Reversibility | Typical Indication | Duration |
|---|---|---|---|
| Composite bonding | Reversible (additive) | Minor chips, small gaps, shape changes | 1–2 visits |
| Porcelain veneers (minimal prep) | Largely irreversible | Colour, shape, size corrections; intact teeth | 2–3 visits |
| Full-coverage crowns | Irreversible | Structurally compromised teeth; heavy bite | 2–3 visits |
| Composite veneers (direct) | Reversible | Budget-conscious; lower durability | 1 visit per arch |
| Gum contouring (gingivectomy) | Irreversible | Gummy smile; uneven gum margins | 1 visit |
| Orthodontics + veneers | Mixed | Misalignment + shape/colour correction | 12–24 months total |
Questions about this procedure?
The Biological Basis of Smile Aesthetics
What makes a smile look natural?
> A natural-looking smile is governed by established proportional relationships: the golden proportion (1:1.618) between adjacent teeth widths, the match between tooth length-to-width ratio (75–80% ideal), the relationship of tooth margins to the gum line, and the alignment of the dental midline with the facial midline. Departures from these proportions are what the eye reads as "wrong" even when the viewer cannot articulate why.
Dental aesthetics are not arbitrary, they operate within biological and evolutionary frameworks that the visual system processes implicitly. The golden proportion and Fibonacci spiral explain the pleasing visual weight of teeth that are proportionally sized to each other and to the face. The gingival architecture, the scalloped contour of the gum tissue around each tooth, mirrors the underlying bone and contributes to the perception of individual tooth form. Teeth that are structurally correct but set in dysharmonic gum architecture appear unaesthetic regardless of their individual restoration quality.
At Stunning Dentistry, our smile design process uses Digital Smile Design (DSD) software to map the patient's facial landmarks, lip mobility, and smile arc to the proposed tooth design before any wax-up or mock-up is produced. This software integration allows us to show the patient a realistic preview of the planned outcome in the context of their own face, not a generic "before and after" but a patient-specific digital simulation that forms the basis of the clinical prescription for the ceramist.
| Aesthetic Parameter | Ideal Range | Common Deviation | Clinical Fix |
|---|---|---|---|
| Tooth length-to-width ratio | 75–80% | Overly wide (worn), overly narrow (tapered) | Veneers with length addition; crown lengthening |
| Central to lateral to canine width | 1.618: 1: 0.618 | Disproportionate laterals; narrow centrals | Veneer reshaping; bonding |
| Dental midline to facial midline | ≤ 2mm deviation acceptable | Significant midline shift | Orthodontic correction first |
| Gingival margin symmetry | Contralateral teeth within 0.5mm | Asymmetric gum margins | Crown lengthening; gum grafting |
| Smile arc | Follows lower lip curvature | Flat arc (reverse curve) | Porcelain length additions |
| Axial inclination | Slight mesial lean | All teeth parallel (artificial) | Veneer shaping; orthodontics |
Ready to discuss your options?
When Smile Design Becomes the Right Approach
When should I consider smile design rather than individual procedures?
> Smile design is the appropriate approach when more than two anterior teeth require aesthetic modification, when the result needs to be planned across multiple teeth with a predictable outcome, when functional concerns (bite, wear, tooth structure) need to be addressed alongside aesthetics, or when the patient's goal is a comprehensive aesthetic transformation rather than a single-tooth correction.
Single-tooth corrections, a chip, a stain, a gap between two adjacent teeth, do not typically require a formal smile design process. They are appropriately managed as individual cases. Smile design becomes the correct framework when the number of teeth involved, the complexity of the aesthetic goal, or the functional concerns (bite changes, tooth wear management, gum architecture) exceed what can be addressed by unplanned individual interventions.
At Stunning Dentistry, no anterior smile design case proceeds past the planning phase without patient approval of a physical mock-up. The mock-up appointment is treated as a diagnostic test, not a formality: if the proposed design requires modification after the patient evaluates it, changes in tooth length, width, colour, or gum display, those modifications are made to the digital plan before preparations begin.
Curious about costs and timelines?

The Digital Smile Design Process
How does digital smile design work?
> Digital smile design (DSD) uses standardised facial and dental photographs mapped to software that allows the clinician to overlay proposed tooth forms on the patient's actual smile. The digital design informs the dental laboratory's wax-up (three-dimensional model of the planned restorations), which is then translated into a temporary mock-up in the patient's mouth for direct evaluation. This sequence links the digital preview to the physical reality before irreversible treatment.
The DSD workflow begins with a specific photography protocol: full-face frontal and three-quarter views at rest and full smile, close-up dental photographs, and, increasingly, 3D intraoral scans. These records establish the baseline facial proportions, lip dynamics, gum-to-tooth ratios, and existing dental anatomy against which the proposed design is mapped. Software tools allow the clinician to trace the midline, smile arc, facial centring lines, and individual tooth outlines, then overlay the proposed tooth design as a vector drawing.
At Stunning Dentistry, our DSD protocol includes video capture of the patient speaking and smiling during the mock-up appointment. This video is reviewed with the patient before any changes are confirmed, the dynamic view of the mock-up in natural speech reveals aspects that static photographs do not. Patients retain digital copies of their pre-treatment records, the DSD overlay, and the approved mock-up for their records.
| DSD Phase | What Occurs | Patient Involvement |
|---|---|---|
| Facial analysis | Photography, DSD software mapping, proportion analysis | Photographs taken; patient reviews overlay |
| Digital design | Clinician maps proposed tooth forms on digital images | Patient approves digital design |
| Wax-up | Ceramist fabricates 3D model of planned restorations | Review of physical model (optional) |
| Mock-up | Temporary material placed in mouth without tooth preparation | Patient evaluates for 30–60 minutes; feedback captured |
| Approval or modification | Design refined based on mock-up feedback | Patient approves; modifications documented |
| Tooth preparation | Preparation begins only after approved mock-up | Irreversible step |
| Temporaries | Temporary restorations matching approved design | Patient evaluates for 1–2 weeks |
| Final ceramics | Laboratory fabricates to approved temporary design | Review at delivery; bonding |
Want a personalised treatment plan?

Treatment Components: What Smile Design Can Include
What procedures are typically part of smile design?
> The most common components are porcelain veneers (for colour and shape correction of intact or minimally damaged anterior teeth), all-ceramic crowns (for structurally compromised teeth), composite bonding (for minor corrections or as a reversible alternative), crown lengthening or gum contouring (for gummy smile or asymmetric gum margins), and teeth whitening as a baseline treatment before matching ceramic shades.
Porcelain veneers are the most commonly used restorative component in anterior smile design. They are thin ceramic facings (0.3–0.7mm) bonded to the labial (front) surface of anterior teeth to change their colour, shape, or apparent position. Traditional veneers require 0.3–0.7mm of enamel reduction to accommodate the ceramic thickness; no-prep or minimal-prep veneers (possible in 15–25% of cases) preserve more tooth structure by using ultra-thin ceramics in cases where no tooth contour reduction is required. Once prepared, veneered teeth require permanent ceramic coverage, there is no reversing tooth reduction.
At Stunning Dentistry, our smile design planning process documents the restoration type selected for each individual tooth and the clinical rationale for that selection. Where a veneer preparation could replace a crown preparation without compromising the aesthetic or structural outcome, we select the less invasive option. Patients receive a tooth-by-tooth treatment map before any preparation begins.
| Component | Best Indication | Tooth Structure Removed | Reversibility |
|---|---|---|---|
| Composite bonding (direct) | Minor chips, small gaps, shape additions | None (additive) | Removable |
| No-prep veneer | Thin, slightly undersized, or retroclined tooth | None or trace | Largely reversible |
| Minimal-prep veneer | Standard colour/shape correction; intact enamel | 0.3–0.5mm enamel | Irreversible |
| Full-prep veneer | Severely discoloured, misaligned | 0.5–0.7mm | Irreversible |
| All-ceramic crown | Structurally damaged, heavily restored, large misalignment | 1.5–2mm circumferential | Irreversible |
| Crown lengthening | Gummy smile; short clinical crowns | Gum and bone tissue | Irreversible |
| Composite veneer (indirect) | Mid-range option; lower ceramic durability | Minimal (similar to veneer) | Irreversible at bonding |
Questions about this procedure?
Materials: Porcelain, Zirconia, and Composite, What Changes
What is the difference between porcelain veneers, zirconia crowns, and composite bonding?
max) provides the best optical match to natural tooth translucency and is the preferred material for anterior veneers and crowns in aesthetic cases. Zirconia is stronger and more resistant to fracture but historically more opaque; layered or monolithic high-translucency zirconia has improved its aesthetic properties. Composite bonding is the most reversible option but less durable than ceramic and subject to colour change and surface wear over time.
Lithium disilicate ceramic (e.max by Ivoclar) is the clinical reference material for anterior smile design. Its layered structure, a reinforced glass-ceramic core with a feldspathic porcelain overlay, replicates the optical gradient from dentine to enamel, allowing the restoration to integrate visually with adjacent natural teeth. Flexural strength (approximately 400 MPa) makes it suitable for single-unit crowns and veneers in the anterior region under normal occlusal loads. It is not indicated in posterior areas carrying heavy biting force, where full-contour zirconia is the preferred material.
At Stunning Dentistry, material selection for each tooth is documented in the treatment plan with the clinical rationale. For standard anterior smile design in patients without parafunction, e.max lithium disilicate is our default veneer and anterior crown material. In patients with documented bruxism or heavy anterior function, we recommend high-translucency zirconia veneers with a diagnostic phase to assess parafunctional risk before committing to any ceramic.
| Material | Flexural Strength | Translucency | Best Use | Durability (Expected) |
|---|---|---|---|---|
| Direct composite bonding | N/A (resin) | Moderate | Reversible trial; minor corrections | 5–8 years before maintenance |
| Indirect composite veneer | ~80–130 MPa | Good | Budget option; low-load anterior | 7–10 years |
| Feldspathic porcelain | ~80–120 MPa | Excellent | Layered veneers; high aesthetic demand | 10–15 years |
| Lithium disilicate (e.max) | ~400 MPa | Very good | Standard anterior veneers and crowns | 15–20+ years |
| Monolithic high-trans zirconia | 650–900 MPa | Good–very good | Bruxism; posterior; high-strength cases | 20+ years |
| Layered zirconia (zirconia+porcelain) | ~600 MPa core | Excellent | Complex anterior crown cases | 15–20 years |
Ready to discuss your options?

Pain and Procedure: What to Expect
Is smile design treatment painful?
> Tooth preparation for veneers and crowns is performed under local anaesthesia, the teeth are anaesthetised before drilling begins. Post-preparation sensitivity to temperature is common for 1–4 weeks after veneer preparation, particularly where enamel is thin or preparation extended close to dentine. Gum contouring produces 3–5 days of mild gum soreness. The final bonding appointment is typically non-surgical and requires only local anaesthesia for sensitivity management.
The preparation appointment for veneers or crowns is the most clinically significant phase of smile design. Under local anaesthetic, the designated amount of enamel (and occasionally dentine) is removed from the tooth surfaces to create space for the ceramic restoration. For minimal-preparation veneers (0.3–0.5mm), the preparation remains within enamel for most of its extent; for full-preparation veneers (0.5–0.7mm) and crowns (1.5–2mm), preparation may extend into dentine, which carries a higher risk of post-preparation temperature sensitivity and a small irreducible risk of pulpal stress.
Between preparation and delivery of the permanent restorations (typically 1–2 weeks), temporary restorations are placed over the prepared teeth. These temporaries replicate the approved mock-up design and serve both a protective and a preview function. Patients experience the planned aesthetic change during daily life, eating, speaking, social interaction, before the permanent restorations are delivered. This evaluation period catches any final adjustments to length, colour, or contour before the irreversible permanent phase.
You should expect temperature sensitivity on prepared teeth during the temporary phase, this is not a sign of pulpal damage but a normal response to enamel reduction exposing dentinal tubules. Sensitivity resolves in the large majority of cases after the permanent ceramic restorations are bonded and the exposed dentine is sealed. Persistent sensitivity beyond 4–6 weeks after final cementation, or spontaneous ache without thermal stimulus, warrants clinical review to assess pulpal status.
At Stunning Dentistry, we use the most conservative preparation depth that achieves the planned aesthetic result for each tooth. All preparations are checked intraoperatively with a calibrated probe to confirm adequate depth without exceeding the planned reduction. Patients receive written information about expected temporary-phase sensitivity and the timeline within which it should resolve before they leave the preparation appointment.
Curious about costs and timelines?

Risk Transparency
What can go wrong with smile design treatment?
> The most clinically significant risks are pulpal stress from preparation (rare but occurs in 1–5% of prepared teeth, potentially requiring root canal treatment), veneer fracture or debonding (more common with porcelain under heavy bite or parafunctional forces), colour or translucency mismatch between adjacent restorations and natural teeth, and patient dissatisfaction with the aesthetic result when the mock-up phase was inadequately conducted or the patient's expectations were not clearly defined.
Preparation-induced pulpal damage is an irreducible risk of any procedure that removes tooth structure. For minimal-preparation veneers that stay within enamel, pulpal risk is very low (< 1%). Full-preparation veneers and crowns, particularly in teeth with larger pulp chambers (younger patients) or teeth with pre-existing sensitivity, carry a higher risk. Pulpal stress may present as transient sensitivity that resolves as the tooth heals, or as irreversible pulpitis requiring root canal treatment. Published rates of pulpal necrosis following elective veneer preparation range from 1–5% over 10 years.
At Stunning Dentistry, all veneer and crown patients complete a bruxism screening questionnaire before treatment planning. Patients with positive screening findings receive a clinical assessment of tooth wear patterns, and material selection is adjusted accordingly. All veneer and crown patients receive a custom occlusal night guard as part of the smile design protocol, fabricated after final cementation to protect the restorations during sleep.
| Risk | Frequency | Trigger | Management |
|---|---|---|---|
| Pulpal stress / necrosis | 1–5% (10-year) | Deep preparation, pre-existing sensitivity | Root canal treatment; no restoration loss |
| Veneer fracture | 3–7% (10-year) | Bruxism, edge-loading, thin incisal ceramic | Material change; night guard; repair or replacement |
| Debonding | 2–5% (5-year) | Inadequate bond preparation; moisture contamination | Re-bonding; check bite |
| Colour mismatch | Case-dependent | Poor shade communication; unrealistic expectations | Return to lab; re-fabricate |
| Gum recession over veneered teeth | < 5% | Preparation margin placement; gum health | Gum graft if significant |
| Tooth sensitivity (permanent) | 5–10% at 1 year | Thin enamel remaining; deep preparation | Desensitising; monitor |
Want a personalised treatment plan?

Clinical Success Determinants
| Success Factor | Why It Matters | What to Verify |
|---|---|---|
| Digital Smile Design and mock-up phase | Prevents aesthetic dissatisfaction; aligns expectations before preparation | Ask whether DSD and physical mock-up are included |
| Conservative preparation philosophy | Minimises pulpal risk and allows future retreatment options | Ask maximum preparation depth planned per tooth |
| Material selection matched to bite force | Bruxism + e.max = fracture risk; must use zirconia | Confirm bruxism assessment is included |
| Ceramist quality and communication | Aesthetic integration depends on ceramic craftsmanship | Ask who fabricates the restorations and their portfolio |
| Shade matching under natural light | Lab shade done under fluorescent light often fails in daylight | Confirm shade is taken and checked under natural light |
| Occlusal equilibration at delivery | High contact spots cause fracture and bite discomfort | Confirm occlusion is checked with articulating paper at delivery |
| Night guard delivery | Protects restorations from nocturnal loading | Confirm night guard is fabricated and delivered post-treatment |
| Gum health before preparation | Gum disease causes recession that exposes preparation margins | Confirm perio is healthy before any smile design begins |
| Informed consent with mock-up approval | Patient must see and approve the result before it is made permanent | Confirm that mock-up approval is a documented clinical gate |
Questions about this procedure?
Longevity and Maintenance
Porcelain and lithium disilicate veneers and crowns have a long clinical record. Published studies consistently report survival rates of 90–95% at 10 years for e.max anterior crowns and veneers in appropriately selected patients. The key determinants of longevity are: absence of uncontrolled parafunction, maintained gum health, adequate ceramic thickness, and correct bonding technique. Veneers that fail are most commonly replaced rather than rendered irreplaceable, the preparation depth typically allows for re-restoration with the same or slightly more coverage.
At Stunning Dentistry, our smile design patients receive a written maintenance protocol including night guard care, flossing technique for veneers, and a recall schedule. We document the shade, material, and bonding agent used for every restoration so that future replacements, wherever performed, can be matched to the established plan.
Ready to discuss your options?
When Smile Design Is Not the Right Approach
Are there cases where smile design is not appropriate?
> Smile design is not the right approach when active periodontal disease, untreated decay, or significant occlusal dysfunction exists, these must be resolved before any aesthetic treatment begins. Patients with active bruxism that is unmanaged, severe dental phobia that prevents restorative procedures, or unrealistic expectations that no achievable aesthetic outcome could satisfy are not candidates for elective ceramic restorations until those conditions are addressed.
Active gum disease is an absolute contraindication to elective veneer and crown preparation. Inflamed gum tissue bleeds when prepared, prevents accurate impression or digital scan records, shifts position unpredictably, and will retract after treatment is complete, exposing preparation margins that the restored gum line was designed to cover. Periodontal treatment, stability confirmation, and a minimum of 3–6 months of healthy gum tissue are required before aesthetic preparation begins.
At Stunning Dentistry, we apply a structured readiness checklist before any smile design preparation is confirmed. This checklist verifies: periodontal health is stable, the patient has reviewed and approved the DSD, the mock-up has been evaluated for a minimum of 30 minutes, the patient has returned the mock-up approval form in writing, and no open questions about the aesthetic outcome remain. The preparation appointment is only booked when all items on this checklist are confirmed.
Curious about costs and timelines?
Reversible vs Irreversible Options
One of the most important clinical distinctions in smile design is between additive (reversible) and subtractive (irreversible) approaches. Composite bonding, added to the tooth surface without preparation, is an additive procedure, the composite can be removed at any point and the tooth is unchanged. No-prep veneers (Lumineers, ultra-thin ceramics) are additive for the small percentage of cases where no reduction is required, approximately 15–25% of candidates in published assessments. All other ceramic veneers and crowns are subtractive: they require removal of tooth structure that cannot be replaced.
At Stunning Dentistry, we assess every anterior smile design case for no-prep and minimal-prep candidacy before planning full-preparation veneers. Where composite bonding achieves 80–90% of the planned aesthetic result with no preparation, we present this as the first option. Where it does not, because the colour correction required exceeds what composite can achieve, or the shade change needed requires ceramic opacity, we present the veneer option with a full explanation of what preparation will involve.
Want a personalised treatment plan?

Cost Logic: CAD Comparison
Materials note: Stunning Dentistry uses IPS e.max (Ivoclar) lithium disilicate and high-translucency zirconia from established global suppliers, the same materials specified by Canadian cosmetic dental laboratories. The cost differential is not a function of ceramic quality but of laboratory fees, dentist overhead, and the significantly higher cost structure of cosmetic dental practice in Canadian major cities.
Timeline note: Most smile design treatments at Stunning Dentistry are completed within a 7–10 day visit: DSD and mock-up on days 1–2, preparation and temporaries on day 3–4, ceramics delivered on days 7–8. Canadian practices typically schedule smile design across multiple appointments over 4–8 weeks.
| Procedure | Stunning Dentistry (India), CAD | Canadian Cosmetic Dentist, CAD | Difference |
|---|---|---|---|
| Single porcelain veneer (e.max) | $350 – $550 | $1,200 – $2,000 | ~$850 – $1,450 saved per tooth |
| Full-arch veneers (8–10 teeth) | $3,000 – $5,000 | $12,000 – $20,000 | ~$9,000 – $15,000 saved |
| Single all-ceramic crown (anterior) | $450 – $650 | $1,200 – $2,200 | ~$750 – $1,550 saved per tooth |
| Composite bonding (4 anterior teeth) | $400 – $800 | $1,500 – $3,000 | ~$1,100 – $2,200 saved |
| Crown lengthening (per site) | $300 – $500 | $800 – $1,500 | ~$500 – $1,000 saved |
| Full smile design (DSD + 10 veneers) | $3,500 – $6,000 | $14,000 – $22,000 | ~$10,500 – $16,000 saved |
Questions about this procedure?
Treatment Comparison Matrix
| Factor | Porcelain Veneers (e.max) | Composite Bonding | All-Ceramic Crowns | Orthodontics |
|---|---|---|---|---|
| Reversibility | Irreversible (preparation) | Reversible (additive) | Irreversible | Reversible |
| Tooth structure removed | 0.3–0.7mm enamel | None | 1.5–2mm circumferential | None |
| Colour correction capacity | Full range | Limited (intrinsic staining) | Full range | None |
| Shape correction capacity | High | Moderate | High | Limited |
| Durability | 15–20+ years | 5–8 years | 15–20+ years | N/A (permanent) |
| Treatment time | 7–14 days (prepared + lab) | 1–2 visits | 7–14 days | 12–24 months |
| Best for | Comprehensive colour + shape change | Minor corrections; uncertain patients | Structurally compromised teeth | Alignment primary issue |
| Cost (CAD, SD) | $350–$550/tooth | $100–$200/tooth | $450–$650/tooth | Varies |
Ready to discuss your options?
Post-Treatment Reality
The period immediately after final ceramic delivery is an adjustment phase. Patients adapt to the new tooth dimensions, which may feel slightly different in speech and tongue position for 1–4 weeks, and the bite is fine-tuned at a review appointment. High contact points identified with articulating paper are adjusted to ensure even, balanced occlusal distribution. This adjustment phase is not a complication; it is an expected and planned component of final delivery.
At Stunning Dentistry, all ceramic restorations are evaluated against the approved mock-up record before bonding. A try-in is performed first in try-in paste without permanent bonding, and the patient confirms the aesthetic outcome under natural light before final cementation proceeds. Any adjustment required at try-in is returned to the laboratory rather than adjusted chair-side, ensuring the final bonded result matches the approved standard.
Curious about costs and timelines?

Common Mistakes
What causes smile design patients to be dissatisfied?
> The majority of smile design dissatisfaction is attributable to insufficient planning, missing or inadequate mock-up, digital design not presented to the patient before preparation, shade communication breakdown between dentist and laboratory, and unmanaged parafunctional habits that lead to early veneer fracture. These are not material failures; they are process failures that a structured planning protocol prevents.
Preparing teeth for veneers without a mock-up is the most preventable cause of dissatisfaction in smile design. Without a physical mock-up worn in the mouth, the patient has no opportunity to evaluate the planned tooth length under natural conditions. Changes in speech patterns, the feel of new incisal edges on the tongue, or dissatisfaction with the smile arc in natural light are only discoverable by wearing the proposed form, not by reviewing digital photographs on a monitor.
At Stunning Dentistry, the treatment plan presented to each smile design patient contains a tooth-by-tooth restoration map with the justification for each choice, the planned preparation depth, the material selected, and the reversibility status. This document is signed by both patient and clinician before preparation proceeds, and forms the clinical record against which the delivered result is evaluated.
Want a personalised treatment plan?
Myth Deconstruction
Myth: "Veneers look fake and obviously dental."
Including additional teeth in a smile design beyond those visible in the patient's smile or requiring aesthetic correction adds cost, complexity, and risk without aesthetic benefit. The planning process should identify which teeth are visible at various smile widths and include only those teeth in the treatment design. Unnecessary preparation of premolars that are not visible at the patient's natural smile width is not a clinical improvement.
Questions about this procedure?
People Also Ask
How many veneers are typically needed for a smile design?
A comprehensive smile design treatment requiring preparation, laboratory fabrication, and permanent bonding is not completed in one visit regardless of technique, the laboratory fabrication of ceramic restorations requires 5–7 working days minimum. Cases involving composite bonding only can be completed chair-side in 1–2 appointments. At Stunning Dentistry, the total treatment period for ceramic smile design is typically 7–10 days, accommodating patients within a single travel visit.
Ready to discuss your options?
Ask Your Doctor
- Is a digital smile design simulation and physical mock-up included in my treatment, and when do I evaluate it?
- What is the planned preparation depth for each tooth, and is minimal-preparation or no-prep possible for any teeth in my plan?
- Who fabricates the ceramic restorations, in-house or at an external laboratory, and can I see their aesthetic work?
- How will shade be selected, and will it be checked under natural light as well as clinical light?
- What material is planned for each tooth, and why was that material chosen over the alternatives?
- Am I a candidate for composite bonding as a reversible first step to evaluate the aesthetic change before committing to ceramics?
- Do I have any bruxism indicators, and how will that affect material selection and post-treatment protection?
- Will I receive a night guard after treatment, and is that included in the cost?
Curious about costs and timelines?

Want a personalised treatment plan?
For Canadian Patients
Pre-Travel Checklist for Canadian Patients Considering Smile Design in India
"addressCountry": "IN"
| Step | Action | When |
|---|---|---|
| 1 | Collect existing dental records (X-rays, previous treatment history) | Before booking travel |
| 2 | Photograph your smile, full-face, close-up, profile, at rest and full smile | Before travel |
| 3 | Send photos and records to Stunning Dentistry for preliminary DSD preview | 4–6 weeks before travel |
| 4 | Ensure gums are healthy; confirm with a Canadian dentist if uncertain | Pre-travel |
| 5 | Disclose any history of grinding, jaw pain, or previous cosmetic dental treatment | Intake form |
| 6 | Plan minimum 10-day visit for full smile design with ceramic restorations | Before booking flights |
| 7 | Arrange local Canadian dentist for post-treatment monitoring; bring treatment records | Post-treatment |
| 8 | Schedule night guard delivery, either at SD before departure or with local dentist post-return | At or shortly after delivery |
Questions about this procedure?
Clinical References
1. Gürel G. "The Science and Art of Porcelain Laminate Veneers." London: Quintessence Publishing, 2003.
*Diagnosis precedes decision.*
Ready to discuss your options?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
Can veneers be placed on teeth that have had root canal treatment?
Root canal treated teeth can receive veneers if they are not structurally compromised to the point of requiring full-coverage crowns. The key assessment is: how much sound coronal tooth structure remains? Teeth with intact labial surfaces and minimal structural damage can be veneered normally. Teeth that are heavily restored, have large post-and-core buildups, or have thin remaining enamel are better candidates for all-ceramic crowns.
What happens if I don't like the final result?
If the delivered ceramic does not match the approved mock-up, this is a legitimate clinical concern. The appropriate response is for the clinician to identify the specific departure from the approved design and either adjust or remake the restoration. Once permanently bonded, remakes require full veneer or crown replacement. This is why the try-in step, evaluation before final bonding, is non-negotiable and must result in patient approval before cementation.
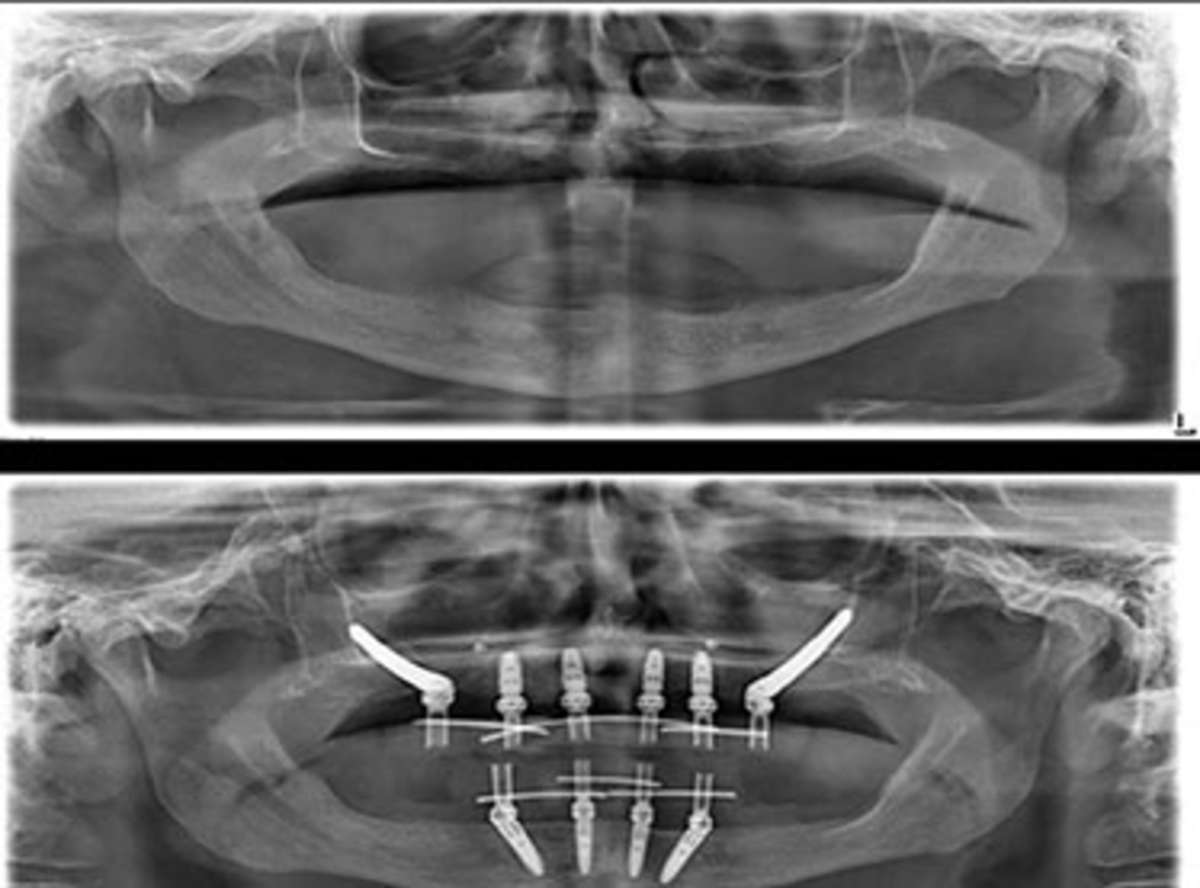
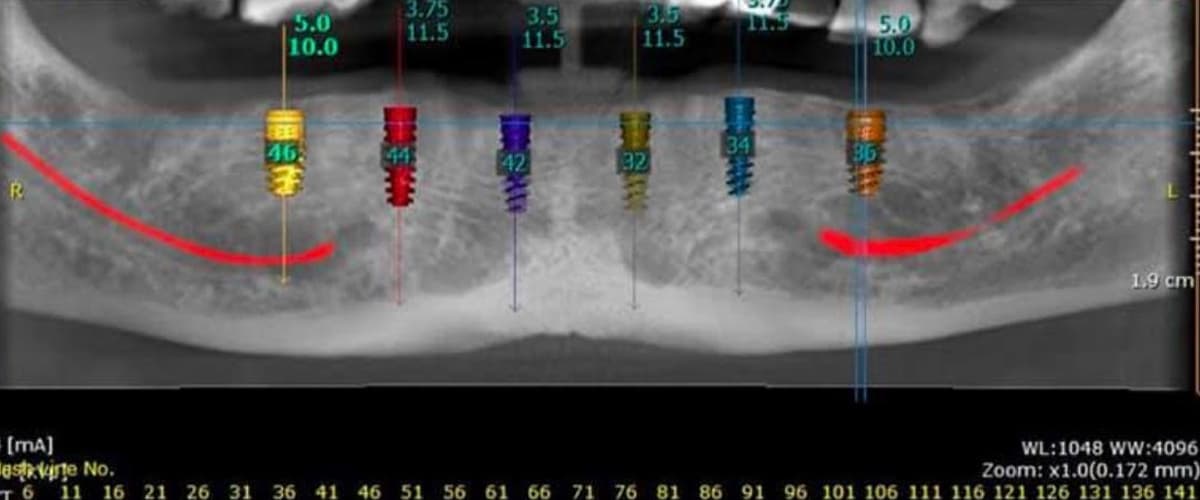
Can smile design be combined with dental implants?
Yes, and frequently is. In patients with one or more missing anterior teeth, the implant crown is designed as part of the overall smile design to integrate seamlessly with the adjacent ceramic veneers or natural teeth. The implant crown shade, contour, and gingival emergence profile are all determined within the DSD planning framework. Implant placement precedes the veneer preparation phase by the implant healing period (3–6 months).
Can I get smile design treatment if I am pregnant?
Elective dental procedures including veneer preparation and ceramic bonding are typically deferred until after delivery to minimise fetal exposure to local anaesthetics and X-ray, and to ensure the patient can lie comfortably in the dental chair for extended appointments. Routine monitoring and emergency treatment proceed normally; elective smile design is scheduled post-partum.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










