Full-Mouth RehabilitationRebuilding Structure, Function, Occlusion, and Aesthetics
- Full-arch implant rehabilitation at Stunning Dentistry costs CAD $10,000–$18,000.
The comparable fee range from a Canadian prosthodontist is CAD $50,000–$80,000.

Full-Arch Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Immediate Load
Full-arch or multiple implant cases where provisional teeth are placed shortly after surgery in suitable clinical conditions.

Multiple Implant Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.

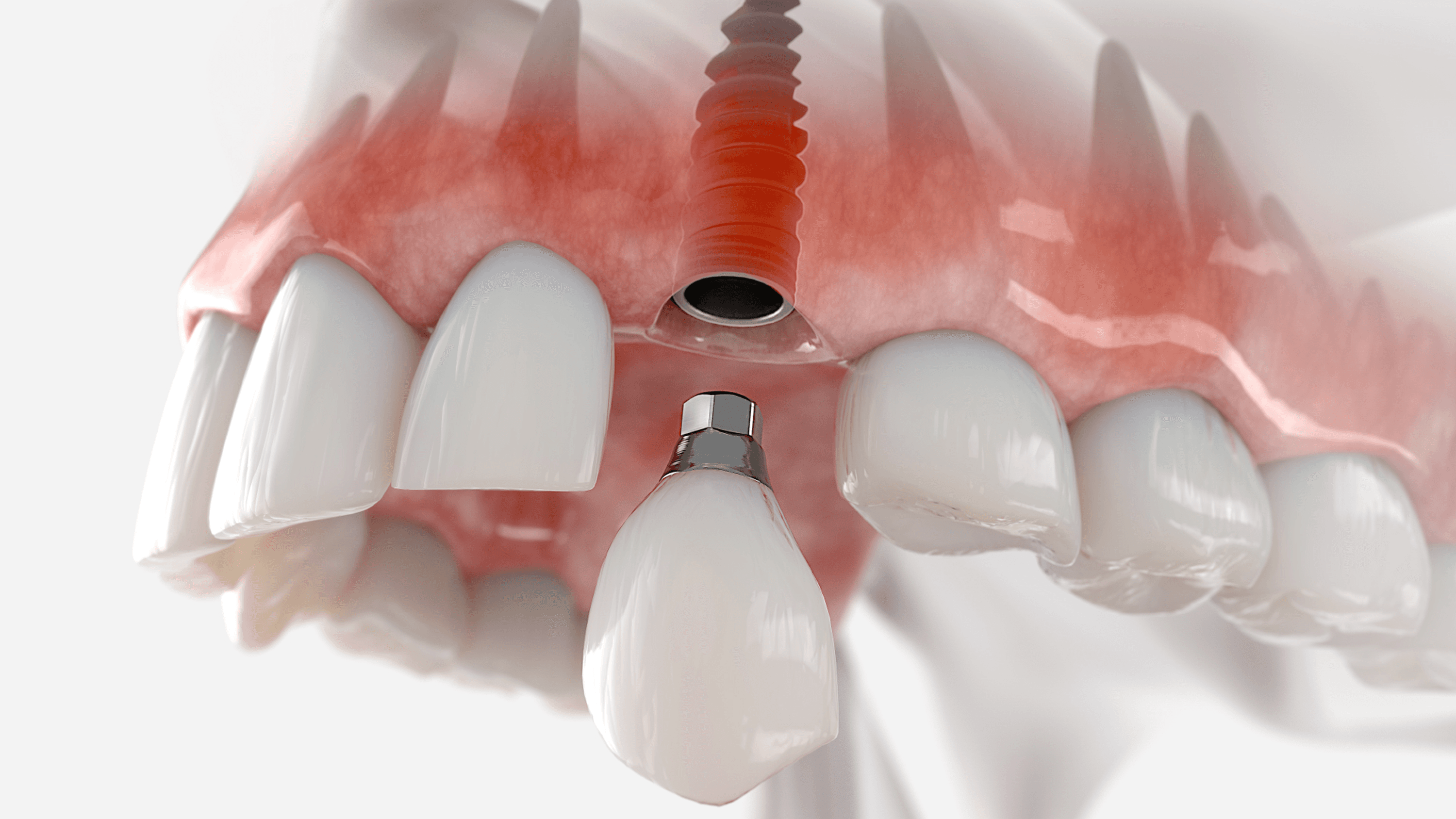
Single Tooth Implant
Single-tooth replacement with an implant and crown for a natural-looking, long-lasting result.

Bone Grafting & Advanced Surgical Support
Regenerative procedures performed to establish adequate bone volume for stable implant placement.

Revision & Complex Implant Cases
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Overview
Full-mouth rehabilitation is the comprehensive reconstruction of every functional tooth surface, or every site where a tooth should be, across one or both dental arches. It is not a single procedure. It is a diagnostic and treatment category that coordinates multiple specialties, sequenced in a defined clinical order, toward a single goal: structural, functional, and occlusal stability across the entire dentition.
At Stunning Dentistry, every full-mouth rehabilitation case begins under protocol SD-FMR-05: dual-clinician sign-off between Dr. Priyank Sethi and a senior prosthodontist before any irreversible treatment proceeds. No implant is placed, no tooth is prepared, no prosthetic is seated without that diagnostic gate being confirmed and documented. This protocol applies to every case, without exception.
| What FMR Addresses | Clinical Classification |
|---|---|
| Every restorable remaining tooth | Tooth-supported restoration: crowns, veneers, inlays, onlays |
| Every non-restorable or missing tooth site | Implant-supported fixed or removable prosthetic |
| Vertical dimension of occlusion | Occlusal rehabilitation, VDO establishment and testing |
| Periodontal support and bone volume | Periodontal treatment and bone augmentation pre-implant |
| Aesthetic architecture | Smile design integrated into the functional treatment plan |
Questions about this procedure?
What Does Full-Mouth Rehabilitation Actually Mean?
What does full-mouth rehabilitation actually mean in clinical terms?
> Full-mouth rehabilitation is the simultaneous or staged reconstruction of every functional tooth surface across one or both dental arches. It addresses structure, occlusion, function, and aesthetics as one coordinated plan, not as separate procedures. Depending on the case, it involves implants, crowns, bone grafting, periodontal treatment, endodontics, and smile design.
Full-mouth rehabilitation is the simultaneous or sequentially staged restoration of every remaining tooth that can be preserved, every missing site that can receive an implant or prosthetic, the vertical dimension of occlusion, the periodontal foundation, and the aesthetic outcome, treated as one integrated clinical problem, not a collection of individual repairs. It is the most coordination-intensive category in clinical dentistry.
At Stunning Dentistry, the first determination in every consultation is whether full-mouth rehabilitation is the appropriate category for this specific case. The diagnostic evaluation establishes whether the patient needs a tooth-supported reconstruction, a full-arch implant protocol, a hybrid combination, or a different pathway entirely. That determination is made from evidence, CBCT imaging, RVG, intraoral scans, mounted study models, and clinical photographs, not from the patient's stated preference or the initial chief complaint.
What Full-Mouth Rehabilitation Is Not
- A single appointment or a quick solution
- A cosmetic procedure that can be reversed if the patient changes preference after the irreversible phase begins
- A treatment that can be planned or quoted before imaging and full clinical examination
- A pathway where one specialist manages all clinical decisions
- An emergency response, it requires diagnostic time, provisional testing, and sequential healing between phases
| FMR Category | What Is Addressed | Typical Protocol |
|---|---|---|
| Full-arch implant | All teeth missing or non-restorable | All-on-4, All-on-6, zygomatic implants |
| Tooth-supported reconstruction | Teeth present but structurally compromised across multiple units | Full-arch crown and veneer preparation, Kois framework |
| Hybrid implant + tooth | Partial edentulism with intact restorable units remaining | Sequenced combination: implants placed, then tooth restorations |
| Overdenture | Full arch with preference for removable prosthetic | 2- or 4-implant retained overdenture |
| Staged orthodontic + restorative | Skeletal or occlusal misalignment affecting load distribution | Orthodontic correction first, then restorative completion |
Ready to discuss your options?
When Is Full-Mouth Rehabilitation Indicated?
When is full-mouth rehabilitation clinically indicated?
> Full-mouth rehabilitation is indicated when structural compromise spans multiple arch segments beyond what targeted single-unit treatment can address. Key indicators include severe tooth wear with lost vertical dimension, advanced periodontal bone loss across multiple units, multiple failed large restorations, congenital structural defects, post-traumatic multi-tooth destruction, or the failure of a prior rehabilitation.
Full-mouth rehabilitation is indicated when the clinical examination reveals that the arch has deteriorated beyond what targeted single-unit treatment can address, when the structural, occlusal, periodontal, or aesthetic damage is distributed across enough of the dentition that treating individual teeth in isolation will not produce a stable or durable outcome. This is a clinical threshold, not a financial one. The indication must be established by examination and imaging, not by the cost of alternatives.
At Stunning Dentistry, candidacy is evaluated against the seven indications above. Every case begins with a comprehensive diagnostic session before any treatment is planned: CBCT for implant assessment, RVG for endodontic and periodontal status, intraoral scans for digital occlusal analysis, and clinical photography in natural light. The diagnostic findings determine the modality, the patient's modality preference is a factor in the discussion, but it does not override the clinical indication.
| Indication | Clinical Presentation | Modality Usually Indicated |
|---|---|---|
| Severe tooth wear | Teeth shortened by attrition or erosion, vertical dimension reduced | Tooth-supported reconstruction, or extraction and implant if too short to restore |
| End-stage periodontitis | Bone loss beyond 50–60% of root length across multiple units | Extractions, bone augmentation, implant-supported |
| Multiple failed large restorations | Fractured or failed crowns, bridges, or large composites across several units | Diagnostic reassessment; hybrid or full-arch depending on remaining tooth viability |
| Congenital structural defects | Amelogenesis imperfecta, dentinogenesis imperfecta, regional odontodysplasia | Case-specific; tooth-supported if structure allows, implant-based if not |
| Post-traumatic destruction | MVA, fall, or sports injury affecting multiple adjacent teeth | Implant or tooth-supported; urgent periodontal and surgical triage first |
| Failed prior rehabilitation | Implant failures, failed fixed bridge, failed denture with bone loss | Salvage assessment, remaining implant evaluation, revised plan |
| Bruxism-related collapse | Occlusal surface attrition, fractured restorations, TMJ dysfunction | Occlusal splint phase first, then VDO restoration, then definitive reconstruction |
Curious about costs and timelines?

The Diagnostic Frameworks That Guide Every Case
What diagnostic frameworks guide full-mouth rehabilitation cases?
> The four principal frameworks are the Dawson Concept, the Kois Technique, the Pankey Philosophy, and the Hobo-Takayama Twin-Stage Technique. Each is grounded in decades of peer-reviewed clinical evidence. The framework selected governs how the bite is analyzed, how jaw position is established, and how the treatment is sequenced from diagnosis to definitive restoration.
Full-mouth rehabilitation without a named diagnostic framework is a sequence of dental procedures without a coherent clinical plan. The frameworks below are not theoretical preferences, they are structured decision-making systems with defined steps for evaluating the bite, establishing jaw position, determining which structures need to change, and sequencing the clinical work to reach a stable, verifiable outcome.
At Stunning Dentistry, every FMR case is governed by a named framework and that framework is documented in the case record. For full-arch implant cases, the Dawson Concept governs centric relation capture and occlusal design. For tooth-supported and aesthetic-driven cases, the Kois 6-step framework structures the case from initial examination through provisional testing and into definitive restoration. The framework selection is made on case type, not preference, and is disclosed to the patient before the treatment plan is finalized.
| Framework | Primary Application | Governing Principle |
|---|---|---|
| Dawson Concept | Full-arch implant and tooth-supported cases | Centric relation as the stable, reproducible mandibular position from which all occlusal design proceeds |
| Kois Technique | Tooth-supported and aesthetic-driven cases | Periodontal, occlusal, structural, and biomechanical risk assessment in a 6-step sequential protocol |
| Pankey Philosophy | Balanced occlusion and phased treatment planning | Anterior guidance development first, posterior occlusal stops second, complexity is staged |
| Hobo & Takayama | Twin-stage technique for long-span or high-risk cases | Complete diagnostic phase and provisional testing before definitive commitment to the restorative plan |
Want a personalised treatment plan?

Core Occlusal Concepts You Need to Understand
What occlusal concepts matter in full-mouth rehabilitation?
> The critical occlusal variables in full-mouth rehabilitation are vertical dimension of occlusion, centric relation, anterior guidance, and the envelope of parafunction. These four parameters govern how the rebuilt bite distributes load, protects restorations, and remains stable over the years following treatment. They must be established and tested in a provisional phase before definitive restorations are placed.
These concepts are the structural grammar of full-mouth rehabilitation. The goal of the provisional phase is to test that the new VDO, the new anterior guidance, and the new occlusal scheme are stable and comfortable before any definitive ceramic or zirconia restoration is fabricated and seated.
| Concept | Clinical Definition | Why It Matters in FMR |
|---|---|---|
| Vertical Dimension of Occlusion (VDO) | The measurable face height when the teeth are in maximum intercuspation | Loss of VDO from wear or tooth loss must be restored, too little space collapses aesthetics and loads the TMJ; too much space causes muscle fatigue and instability |
| Centric Relation (CR) | The position of the mandibular condyle in the glenoid fossa when the jaw is in its most superior, anterior, and stable position | The jaw position from which the entire occlusal design is constructed, all bite records, articulator settings, and provisional trials reference this position |
| Maximum Intercuspation (MIP) | The tooth position where the greatest number of upper and lower teeth are in contact | In most patients, CR and MIP do not coincide, FMR establishes a stable MIP that is coincident with or close to CR |
| Anterior Guidance | The pathway the upper anterior teeth provide for lower teeth during lateral and protrusive jaw movement | Protects posterior teeth and restorations from destructive lateral forces; must be designed deliberately in FMR, not left to chance |
| Canine-Protected Occlusion | The canine teeth bear lateral force and disocclude posterior teeth on lateral movement | Preferred guidance scheme in most FMR cases, simplest to design, most protective of posterior restorations |
| Envelope of Parafunction | The range of jaw movements during non-functional activity, bruxism, clenching | Determines the mechanical stress the rehabilitation must be designed to survive; night guard management is part of every bruxism-related FMR case |
| Posselt's Envelope of Motion | The three-dimensional boundary of all possible mandibular movement | Used to verify that the new VDO and occlusal scheme fall within the physiologically tolerable range |
| Christensen Phenomenon | The space that opens between posterior teeth during protrusive jaw movement | Must be accounted for in full-arch occlusal design to prevent leverage forces on anterior implants |
Questions about this procedure?
The Five Modalities of Full-Mouth Rehabilitation
What are the five main modalities of full-mouth rehabilitation?
> The five modalities are: full-arch fixed implant prosthetics (All-on-4, All-on-6, zygomatic), full-mouth tooth-supported crown and veneer reconstruction, hybrid implant-plus-tooth combination cases, implant-retained overdentures, and staged orthodontic-plus-restorative treatment. The modality is determined by bone volume, remaining tooth viability, occlusal condition, and patient medical profile, not by patient preference alone.
Full-mouth rehabilitation encompasses five distinct modalities. Each modality addresses a different clinical starting point and produces a different prosthetic outcome. The decision between modalities is made on bone volume, remaining tooth viability, occlusal and periodontal status, and the patient's systemic health and surgical risk tolerance. No single modality is superior across all cases, the right modality is the one the diagnostic examination indicates.
The linked sub-pages cover each modality in clinical depth: implant angulation, bone considerations, immediate loading criteria, material selection, and the specific Canada-versus-India cost comparison per modality.
| Modality | Indications | Typical Timeline at Stunning Dentistry |
|---|---|---|
| Full-arch fixed implant (All-on-4 / All-on-6) | All or most teeth non-restorable, adequate bone volume | 7–10 days: extraction + implant + temporary fixed prosthetic; definitive at 4–6 months |
| Zygomatic implant | Severely resorbed upper jaw with insufficient bone for standard implants | 7–10 days: zygomatic placement + immediate loading; no bone graft phase |
| Tooth-supported crown and veneer FMR | Multiple teeth restorable, structural compromise but viable roots | 7–10 days: preparation, temporisation, impression; definitive at 4–6 weeks |
| Hybrid implant + tooth | Partial edentulism with intact restorable units | Sequenced: implants first, tooth preparations after osseointegration confirmed |
| Implant-retained overdenture | Full arch, patient preference for removable, or cost-limited | 2–4 implants placed; definitive overdenture at 3–4 months |
Ready to discuss your options?

All-on-4 Full-Arch Fixed
Full-arch fixed rehabilitation using 4 implants per arch is the most widely documented immediate-loading protocol in implant dentistry. Two implants are placed axially in the anterior zone; two are placed at a 30–45° posterior angulation to maximize implant distribution and reach denser anterior bone while avoiding the inferior alveolar nerve or the maxillary sinus, depending on the arch.
Curious about costs and timelines?

All-on-6 When Bone Allows
All-on-6 adds two additional implants to the All-on-4 base protocol where posterior bone volume is sufficient for axially placed additional implants. The added implants improve load distribution, reduce cantilever stress on posterior prosthetic segments, and increase long-term prosthetic stability, particularly relevant in the mandible where chewing forces are highest.
Want a personalised treatment plan?
Zygomatic When Bone Is Gone
Zygomatic implants bypass the severely resorbed upper jaw entirely. The implant is anchored in the zygomatic bone, the cheekbone, which retains sufficient volume even after years of maxillary bone loss. The technique eliminates the need for bone grafting and the 6–12-month graft-healing delay that precedes conventional implant placement in resorbed upper jaws.
Questions about this procedure?

Teeth-in-a-Day: Immediate Loading
Teeth-in-a-Day is the clinical and marketing term for same-day full-arch implant placement and immediate loading, the patient leaves the surgery with a fixed full-arch temporary prosthetic in place. It is not a different implant system. It is a loading protocol applied to either All-on-4 or All-on-6 implant placement, contingent on achieving sufficient primary stability at placement.
Ready to discuss your options?

Smile Design for Aesthetic-Led Cases
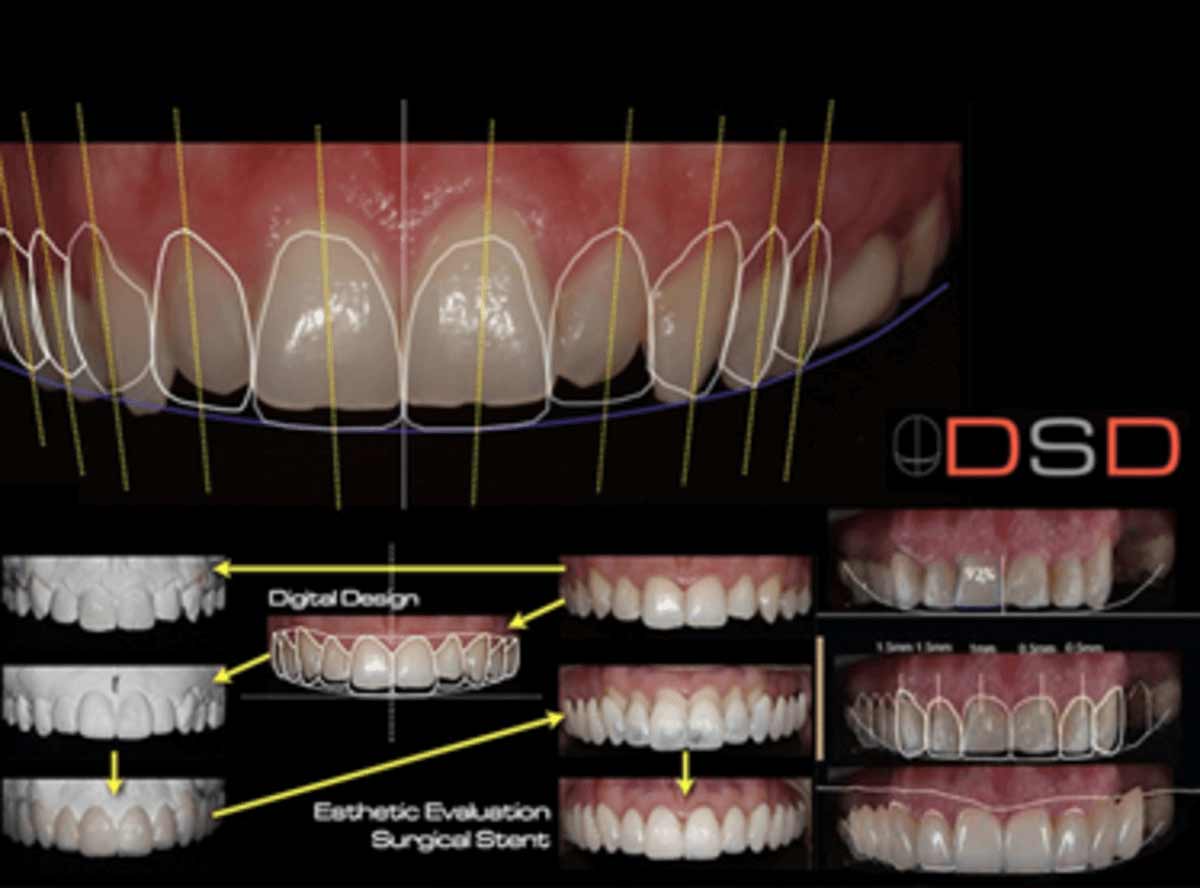
Full-mouth rehabilitation that begins with an aesthetic goal, tooth shade, shape, proportion, smile architecture, requires that the aesthetic plan be subordinated to the functional plan, not the reverse. Digital smile design tools (DSD, 3Shape Smile Design) produce a preview of the intended aesthetic outcome; that preview is then translated into wax-up and provisional form for patient approval before any irreversible tooth preparation begins.
Curious about costs and timelines?

Full-Mouth Tooth-Supported Rehabilitation
When sufficient tooth structure remains, roots intact, periodontal support adequate, pulp health confirmed, tooth-supported full-mouth rehabilitation uses the patient's own teeth as the foundation for a complete restorative reconstruction. Full-coverage crowns, partial coverage onlays, veneers, and inlays are selected per tooth based on the structural analysis. No implants are placed. No surgery is involved.
Want a personalised treatment plan?
The Interdisciplinary Team: Who Does What
Full-mouth rehabilitation is inherently a multi-specialist undertaking. No single clinician, regardless of training, can perform every procedure a complex FMR case may require at the standard each specialty demands. The interdisciplinary team structure is the mechanism by which each component of the case is executed by the clinician with the deepest specific competence in that component.
| Specialist | Role in FMR | When They Are Involved |
|---|---|---|
| Prosthodontist | Case planning, occlusal design, crown and bridge fabrication, implant restoration, final prosthetics | Leads the case from diagnosis through definitive restoration |
| Periodontist | Gum health assessment, bone grafting, sinus lifts, implant site preparation, soft tissue surgery | Before implant placement; ongoing in tooth-supported cases |
| Oral Surgeon / Implantologist | Tooth extraction, implant placement (All-on-4, All-on-6, zygomatic), ridge preservation | Surgical phase |
| Endodontist | Root canal treatment on teeth to be retained; assessment of pulp viability | Before tooth preparation in tooth-supported cases |
| Orthodontist | Space management, arch form correction, bite normalisation before restorative | Cases where teeth or arch form need repositioning before restoration |
| TMJ and Pain Specialist | Bite splint therapy, TMD management, bruxism protocol | Cases involving pain, clicking, limited opening, or bruxism before or during rehabilitation |
| Laboratory Technician | Wax-ups, provisionals, digital mock-ups, fabrication of definitive restorations | Throughout; particularly critical in the provisional phase |
| Radiologist / CBCT Reader | Bone volume, sinus anatomy, nerve mapping, implant site analysis | Diagnostic phase |
Questions about this procedure?

The Digital Workflow: 2025–2026 Standard
What digital technology is used in full-mouth rehabilitation today?
> Contemporary full-mouth rehabilitation uses intraoral scanning for digital impressions, CBCT for 3D bone mapping, CAD/CAM software for prosthetic design, digital face bow and virtual articulator for bite simulation, and PMMA-milled provisionals for function testing before any ceramic or zirconia definitive is fabricated.
The digital workflow in full-mouth rehabilitation replaces or augments the traditional analog sequence at each stage where digital precision improves accuracy, reduces chair time, or reduces laboratory error. The transition to digital has not changed the diagnostic framework, it has changed how diagnostic data is captured, stored, and transmitted to the laboratory, and how provisional and definitive restorations are designed and fabricated.
At Stunning Dentistry, the digital workflow includes intraoral scanning (Trios 4 or Medit), CBCT-based implant planning, CAD-CAM design for provisional and definitive restorations, and virtual articulator simulation before any irreversible preparation begins. PMMA-milled provisionals are fabricated for every full-arch case and worn for a minimum of 4–6 weeks before the definitive is approved for fabrication.
| Digital Tool | Purpose | Stage in FMR |
|---|---|---|
| Intraoral Scanner (Trios / Medit) | Full-arch digital impression; occlusal record | Diagnostic and restorative phases |
| CBCT (Carestream / Planmeca) | Bone volume, sinus, nerve, implant site analysis | Diagnostic phase |
| Implant Planning Software (Simplant / coDiagnostiX) | Surgical guide design; virtual implant placement | Pre-surgical phase |
| Digital Face Bow / Virtual Articulator | Condylar pathway; occlusal simulation; excursive movement | Diagnostic and provisional phase |
| CAD/CAM Design (3Shape / exocad) | Prosthetic design: crowns, bridges, full-arch prosthetics | Laboratory phase |
| PMMA Milling | Functional provisional fabrication | Provisional testing phase |
| Milling Centre (Zirconia / e-max) | Definitive restoration fabrication | Final restorative phase |
Ready to discuss your options?
Materials Used for the Definitive Rehabilitation
Definitive material selection in full-mouth rehabilitation is governed by the biomechanical demands of each arch position, the aesthetic requirements of the case, and the opposing occlusal material. The material cannot be selected before the modality is selected, and the modality cannot be selected before the diagnostic examination is complete.
| Material | Classification | Primary Application | Key Property |
|---|---|---|---|
| Monolithic Zirconia (5Y-TZP) | Full-contour ceramic | Posterior full-arch fixed prosthetics; implant-supported bridges | Highest fracture resistance; suitable for bruxism cases |
| Lithium Disilicate (e-max) | Glass-ceramic | Anterior crowns and veneers; aesthetic-priority zones | Excellent light transmission; superior aesthetics to zirconia |
| PEKK (Poly-ether-ketone-ketone) | High-performance polymer | Provisional full-arch prosthetics; shock-absorbing frameworks | Resilient under load; reduces implant-level stress |
| PMMA (acrylic) | Resin | Interim full-arch provisionals; function-testing phase | Machineable; inexpensive; easily adjusted |
| Titanium Framework | Metal | Implant bar frameworks for full-arch fixed bridges | Dimensional stability; long-term prosthetic foundation |
| Straumann SLActive / BLX | Implant | All-on-4, All-on-6, primary stability cases | Hydrophilic surface; accelerated osseointegration |
| Nobel Biocare Active | Implant | Immediate loading cases; high primary stability requirements | Tapered design; aggressive thread for initial torque |
| Osstem TSIII / USIII | Implant | Value-tier; CBCT-guided placement | Documented survival; cost-effective for combination cases |
| Ivoclar Vivadent IPS Empress | Pressed ceramic | Anterior veneers and inlays | Shade accuracy; layered pressed technique |
| 3M ESPE Lava | Zirconia | Posterior bridgework | Well-documented; high translucency options |
Curious about costs and timelines?

The Evidence Base for Full-Mouth Rehabilitation
What does the evidence say about full-mouth rehabilitation outcomes?
> Long-term evidence supports full-mouth rehabilitation as durable and predictable when executed under interdisciplinary protocols and named diagnostic frameworks. Implant survival rates for full-arch protocols (All-on-4, All-on-6) exceed 95% at 5 years in peer-reviewed cohort data. Tooth-supported FMR shows similar durability when periodontal foundation is confirmed and provisional testing precedes definitive placement.
Full-mouth rehabilitation has an evidence base spanning more than five decades of peer-reviewed clinical research. The volume, function, and longevity outcomes for implant-supported full-arch prosthetics are among the most studied topics in contemporary prosthodontic literature. The evidence supports the procedure, what it does not support is execution outside a defined diagnostic and clinical standard.
At Stunning Dentistry, clinical decisions are referenced against the peer-reviewed literature in implantology (Journal of Oral Implantology, Clinical Oral Implants Research), prosthodontics (JPD), and endodontics (JOE). We do not cite internal outcome data as equivalent to peer-reviewed studies. We apply published evidence to clinical decisions and explain the evidence basis to patients when asked.
| Evidence Source | Primary Journal | Relevant Metric |
|---|---|---|
| All-on-4 cohort data | Clinical Oral Implants Research | Implant survival, prosthetic complications, bone loss at 5 years |
| FMR occlusal outcomes | Journal of Prosthetic Dentistry | Restoration survival, retreatment rates, patient satisfaction |
| Periodontal impact on implant outcomes | Journal of Periodontology | Pre-implant periodontal control and peri-implantitis incidence |
| Zygomatic implant outcomes | International Journal of Oral & Maxillofacial Implants | Survival in resorbed maxilla; complication profile |
| Digital workflow accuracy | International Journal of Prosthodontics | Fit accuracy of CAD/CAM vs conventional prosthetics |
Want a personalised treatment plan?

Candidacy: Medical, Dental, and Psychological
Who is a good candidate for full-mouth rehabilitation?
> The ideal candidate has a stable systemic medical condition, adequate or augmentable bone volume for the chosen modality, periodontal disease either resolved or controlled, realistic expectations about the multi-phase treatment timeline, and the capacity to maintain the result with regular home care and annual reviews. Medical, dental, and psychological candidacy are each assessed before treatment is approved.
Candidacy for full-mouth rehabilitation requires assessment across three dimensions: medical, dental, and psychological. A patient who meets all medical and dental criteria but whose expectations are not aligned with what the procedure can deliver will have a poor outcome not because the clinical work failed but because the goal was never achievable through dental treatment alone.
At Stunning Dentistry, medical candidacy is assessed at the diagnostic appointment. Where systemic conditions require specialist liaison, we coordinate directly with the patient's treating physician or specialist before the treatment plan is finalised. We do not proceed with implant surgery in patients with uncontrolled systemic disease. Candidacy decisions are documented in the case record.
| Candidacy Factor | Assessment Method | Common Management |
|---|---|---|
| Bone volume | CBCT, bone height, width, density, sinus anatomy | Bone augmentation, sinus lift, zygomatic protocol if insufficient |
| Periodontal status | Probing, bone level radiographs, mobility assessment | Periodontal treatment completed before implant placement |
| Diabetes control | HbA1c review; GP liaison | Stabilisation to HbA1c ≤7–8% before implant surgery |
| Smoking | Patient history | Cessation protocol before and after surgery |
| Bisphosphonates | Medication history; oncology liaison if IV | Risk stratification; drug holiday assessment per protocol |
| Bruxism | Clinical wear pattern; occlusal splint response | Night guard therapy before and after rehabilitation |
| Psychological expectations | Clinical interview; documented | Alignment of patient expectations with achievable outcomes before treatment proceeds |
Questions about this procedure?
Full-Mouth Rehabilitation Modalities Compared
How do the full-mouth rehabilitation modalities compare to each other?
> The five modalities differ primarily in bone requirement, reversibility, prosthetic permanence, maintenance demands, and total cost. Fixed implant prosthetics offer the most stable long-term outcome and the lowest maintenance burden but require adequate bone and surgical eligibility. Tooth-supported reconstruction preserves natural dentition but requires sufficient structural viability across every retained tooth.
A modality comparison is informational. It is not a substitute for a diagnostic examination. The table above shows typical ranges, your specific case may fall inside or outside these ranges depending on bone volume, case complexity, number of implants required, and material selection.
| Factor | Full-Arch Fixed Implant | Tooth-Supported FMR | Hybrid Implant + Tooth | Overdenture | Staged Ortho + Restorative |
|---|---|---|---|---|---|
| Bone requirement | Moderate–high | None | Moderate | Low (2–4 implants) | None |
| Surgery required | Yes | No | Yes (partial) | Yes (minimal) | No |
| Reversibility after surgery | No | Partial (crowns removable) | No | Yes (removable) | Partial |
| Prosthetic permanence | Fixed, permanent | Fixed on remaining teeth | Fixed on implants, fixed on teeth | Removable at night | Fixed after ortho completion |
| Maintenance demand | Annual review; 5-year prosthetic check | Regular dental hygiene; 6-monthly checks | Combination of above | Attachment servicing; denture relining | Standard restorative maintenance |
| Typical timeline at SD | 7–10 days + 4–6 months for definitives | 7–10 days + 4–6 weeks for definitives | Sequenced: 2 visits | 2 visits: implant + definitive overdenture | 2–3 visits over treatment arc |
| CAD cost range (Stunning Dentistry) | $10,000–$18,000 per arch | Case-specific | Case-specific | Case-specific | Case-specific |
| CAD cost range (Canadian prosthodontist) | $50,000–$80,000 per arch | $25,000–$60,000 | $35,000–$70,000 | $15,000–$30,000 | $20,000–$50,000 |
Ready to discuss your options?
What Determines the Cost of Full-Mouth Rehabilitation?
What determines the cost of full-mouth rehabilitation?
> Cost is determined by modality (implant vs tooth-supported), number of implants, number of arches treated, bone augmentation requirements, implant brand tier, material selection for the definitive prosthetic, and the number of specialist visits required. A single-arch All-on-4 with standard bone volume costs significantly less than a bilateral zygomatic case with additional bone augmentation.
These factors are assessed at the diagnostic appointment. The treatment plan produced after the diagnostic session will itemise each component and its associated cost. A quote issued before the diagnostic session is an estimate, not a treatment plan.
| Cost Factor | Lower Cost | Higher Cost |
|---|---|---|
| Number of arches | Single arch | Both arches |
| Implant count | 4 implants (All-on-4) | 6–8 implants (All-on-6 or zygomatic) |
| Bone augmentation | No graft required | Sinus lift or major bone augmentation |
| Implant brand | Osstem TSIII | Straumann SLActive or Nobel Biocare |
| Prosthetic material | PMMA long-term temporary | Monolithic zirconia or titanium-framed |
| Provisional phase | Short (4–6 weeks) | Extended (6–12 months for complex VDO changes) |
| Specialist involvement | Single-arch, standard anatomy | Multi-specialist team: oral surgery + perio + endo + prosth |
| Aesthetic demands | Functional priority | Full-aesthetic zone treatment (anterior veneers, smile design) |
Curious about costs and timelines?
Canadian Specialist Quotes vs Stunning Dentistry Pricing
How does Stunning Dentistry's cost compare to Canadian prosthodontists?
> A full-arch implant rehabilitation at a Canadian prosthodontist costs CAD $50,000–$80,000 per arch in private practice. The same protocol at Stunning Dentistry costs CAD $10,000–$18,000 per arch, with a 10-year written warranty. The cost differential funds the return flight, accommodation, and a substantial reserve, most Canadian patients pay significantly less in total even after travel expenses are included.
The cost difference is not driven by inferior materials, lower clinical standards, or less experienced clinicians. It is driven by the cost of specialist time, laboratory fees, facility overhead, and malpractice insurance in the Canadian private dental market. The clinical protocols, implant brands, prosthetic materials, diagnostic frameworks, are internationally consistent at a clinic operating to the standard Stunning Dentistry operates to.
| Cost Component | Canadian Prosthodontist (private practice) | Stunning Dentistry (India) |
|---|---|---|
| Full-arch implant protocol (4 implants + fixed prosthetic) | CAD $50,000–$80,000 | CAD $10,000–$18,000 |
| Flight (Toronto/Vancouver to New Delhi return) | N/A | ~CAD $1,200–$2,000 |
| Accommodation (7–10 days) | N/A | ~CAD $700–$1,400 |
| Total out-of-pocket (approximate) | CAD $50,000–$80,000 | CAD $12,000–$21,400 |
| Canadian wait time for consultation + treatment | 3 months–1 year | 7–10 clinical days |
| Warranty | Varies by practice | 10-year written warranty, signed and dated |
| Post-treatment follow-up access | Local | Annual review; 10-year open file; remote consultation available |
| Coverage under Canadian provincial insurance | Typically excluded (cosmetic) | Not applicable |
Want a personalised treatment plan?

Step-by-Step: How Full-Mouth Rehabilitation Runs at Stunning Dentistry
What does the full-mouth rehabilitation process look like step by step?
> The process runs in three gates: diagnostic, provisional, and definitive. The diagnostic gate includes imaging, examination, case planning, and patient approval. The provisional gate includes surgical and initial restorative work with a temporary prosthetic worn for 4–6 weeks to test function and comfort. The definitive gate converts the tested provisional outcome to ceramic or zirconia permanence.
Full-mouth rehabilitation does not begin with surgery. It begins with a diagnostic phase that determines what the surgery, if any, should accomplish. The three-gate structure below applies to implant-supported full-arch cases. Tooth-supported cases follow a similar sequence without the surgical phase.
Gate 1, Diagnostic Phase (Day 1–2)
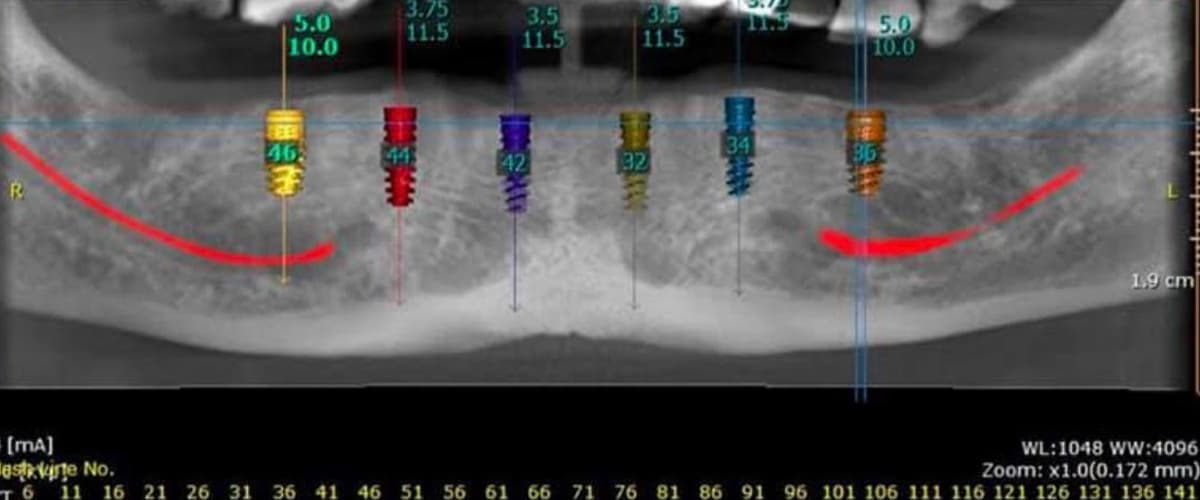
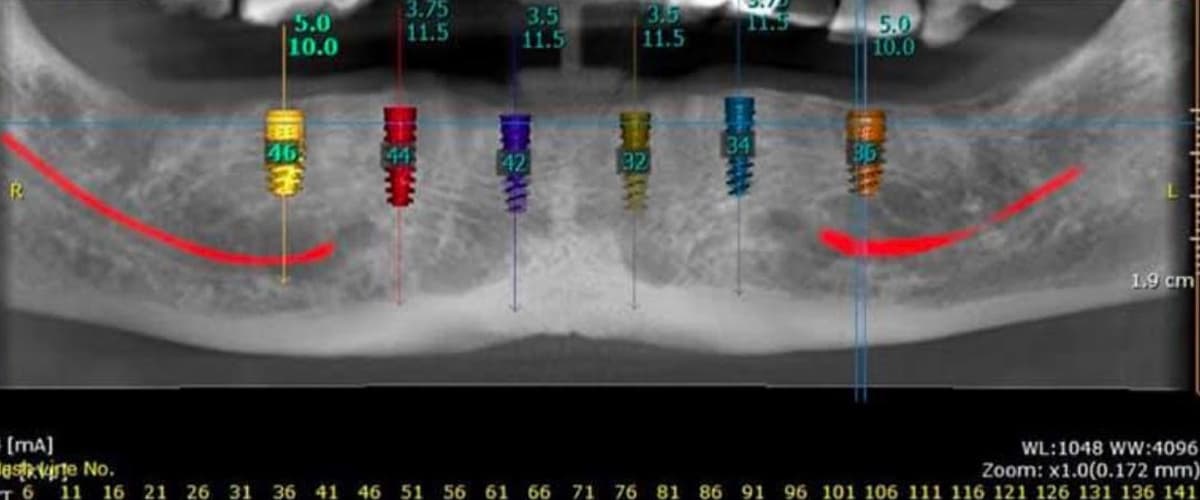
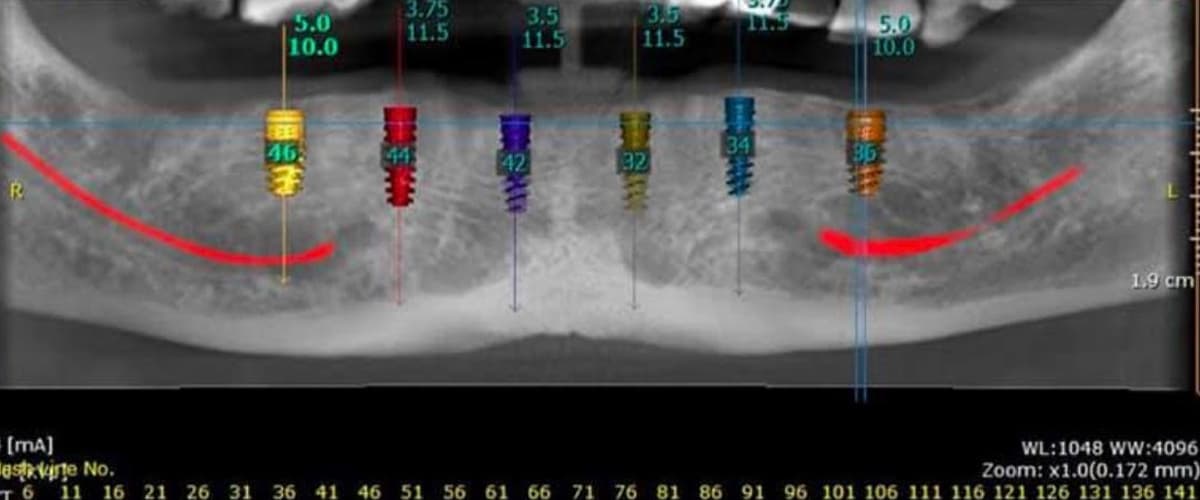
1. CBCT scan for bone volume, sinus, and nerve mapping
2. RVG (periapical radiographs) for endodontic and periodontal status of remaining teeth
3. Intraoral scan: full arch digital impression and occlusal record
4. Clinical photography: facial, profile, retracted, bite
5. Periodontal charting: probing depths, mobility, furcation involvement
6. TMJ and occlusal assessment: condylar position, range of motion, signs of dysfunction
7. Diagnostic wax-up or digital mock-up: proposed prosthetic outcome
8. Three-stage patient approval: diagnostic findings presented, treatment plan presented, informed consent for irreversible procedures obtained
No irreversible procedure is planned before Gate 1 is complete and all three approval stages are signed by the patient.
Gate 2, Surgical and Provisional Phase (Day 3–7)
9. Extractions of non-restorable teeth (if indicated) under local anaesthesia, with sedation option available
10. Implant placement: All-on-4, All-on-6, or zygomatic protocol under protocol SD-FMR-05 dual-clinician sign-off
11. Immediate loading: full-arch PMMA provisional fixed prosthetic placed on the day of surgery (if primary stability criteria are met)
12. RVG post-surgical confirmation
13. Soft diet protocol briefing; oral hygiene instruction; night guard fitting if bruxism
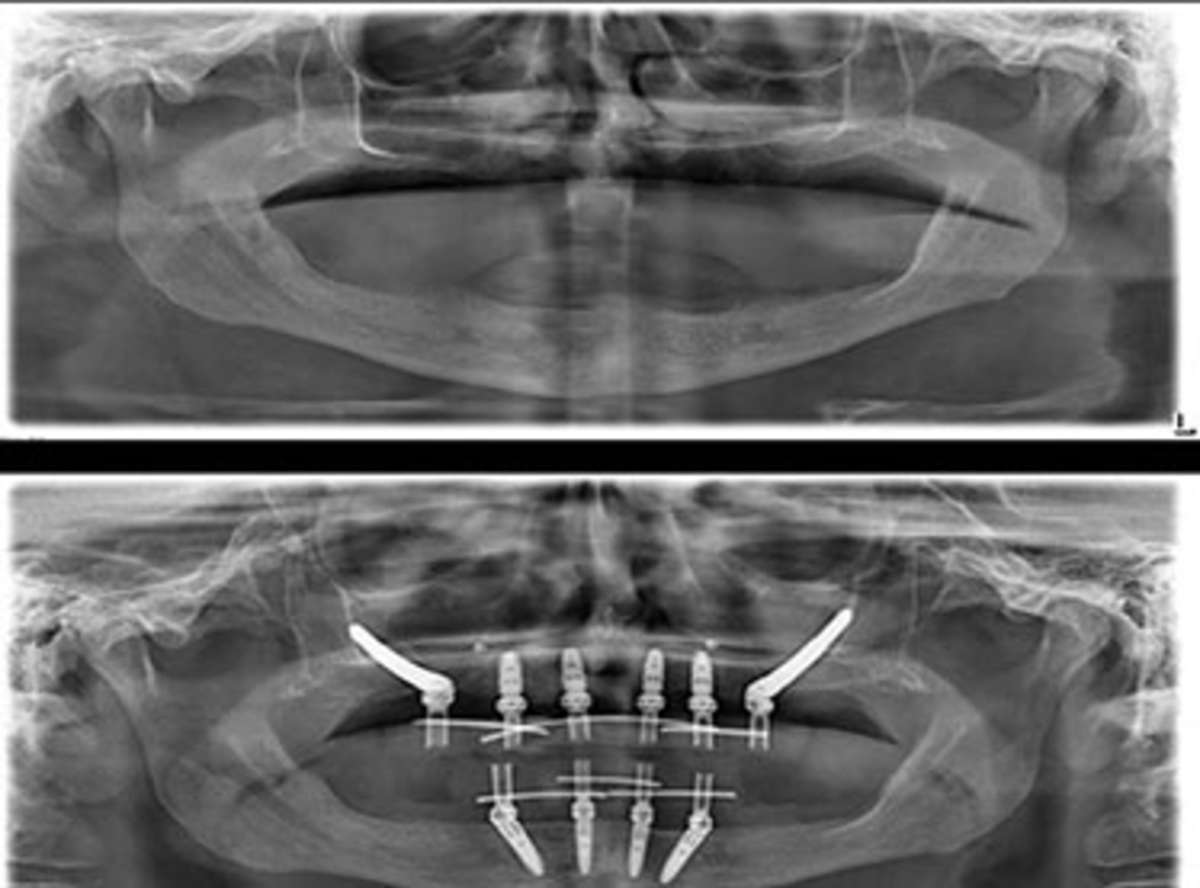
Gate 3, Definitive Phase (4–6 months post-implant; 4–6 weeks post-tooth-prep)
14. Healing and osseointegration confirmed by clinical and radiographic assessment
15. Definitive impressions or intraoral scans for final prosthetic fabrication
16. Laboratory fabrication: monolithic zirconia, lithium disilicate, or hybrid titanium-ceramic framework
17. Definitive seating: torque verification; aesthetic and occlusal confirmation; final documentation
18. Warranty issued: 10-year written warranty signed, dated, and filed; review schedule at 1, 3, 5, 10 years confirmed
| Phase | When | What Happens |
|---|---|---|
| Diagnostic Gate | Day 1–2 | Imaging, examination, digital mock-up, patient approval |
| Surgical Gate | Day 3–5 | Extractions, implant placement, immediate provisional |
| Healing Period | Months 1–4 | Osseointegration; provisional testing; dietary restrictions |
| Definitive Gate | Month 4–6 | Final impressions, prosthetic fabrication, seating |
| Warranty Issued | At definitive seating | 10-year written warranty; review schedule |
Questions about this procedure?
Aftercare and Long-Term Maintenance
What maintenance does full-mouth rehabilitation require long-term?
> Full-mouth rehabilitation requires annual professional maintenance for implant-supported cases: peri-implant tissue assessment, radiographic bone level check, prosthetic torque verification, and hygiene cleaning. Tooth-supported cases require 6-monthly hygiene appointments. All cases require a night guard if bruxism is present. The 10-year written warranty at Stunning Dentistry covers issues traceable to clinical work, it does not replace home care.
Osseointegration is biological, not guaranteed. Once the implant is in place and the prosthetic is seated, the long-term outcome depends on two variables the clinic cannot control after the patient returns home: bone health and oral hygiene. Peri-implantitis, inflammation around the implant, is the primary late complication of implant-supported rehabilitation, and it is a hygiene-related condition. It is preventable; it is not self-limiting once established.
At Stunning Dentistry, every patient leaves with a written aftercare protocol, a direct communication channel for questions about postoperative concerns, and a confirmed follow-up schedule. The 10-year open file means that any patient who returns for the year-1, year-3, year-5, or year-10 review will have their complete diagnostic and treatment record available. If a year-10 review surfaces a problem traceable to Stunning Dentistry's clinical work, the fly-back-eligible clause of the warranty applies.
| Maintenance Task | Frequency | Who Performs It |
|---|---|---|
| Professional hygiene (implant-specific instruments) | Every 6 months | Local Canadian dental hygienist / dentist |
| Peri-implant radiographic bone level check | Annually | Local Canadian dentist or periodontist |
| Prosthetic screw torque verification | Annually for the first 2 years; then as needed | Local Canadian dentist with implant driver kit |
| Night guard replacement or adjustment | When signs of wear appear | Local Canadian dentist |
| Stunning Dentistry scheduled review | Year 1, 3, 5, 10 | At Stunning Dentistry; remote video option available |
Ready to discuss your options?
Myths vs Clinical Reality
| Myth | Clinical Reality |
|---|---|
| "Full-mouth rehabilitation is just for people who want a perfect smile." | FMR is indicated by structural, functional, and periodontal criteria, not aesthetic ambition. Many patients pursue FMR because they cannot eat properly, not because of dissatisfaction with appearance. |
| "Dental implants last a lifetime." | Implants can last for decades. They are not lifetime-guaranteed biological structures. Peri-implantitis, prosthetic wear, and bone changes can affect implants over time. Proper maintenance significantly extends longevity. |
| "Getting dental work done in India is risky." | The risk profile is determined by the clinical protocols, the diagnostic standards, the sterilisation practices, and the experience of the clinical team, not by the country. A clinic operating to international standards in India is safer than a clinic ignoring standards anywhere. |
| "If something goes wrong, I'll be stranded." | The appropriate question is: what is the complication management protocol? Stunning Dentistry maintains a 10-year open file, provides remote consultation access, and the warranty includes fly-back eligibility for complications traceable to clinical work. |
| "The cheaper price means cheaper materials." | Material cost in dental rehabilitation is a fraction of total treatment cost. Straumann implants, e-max, and monolithic zirconia are available to clinics in India at the same wholesale cost as in Canada. The price differential reflects specialist labour, facility, and insurance cost differences, not material differences. |
| "I can go for a consultation and decide later." | For implant cases, the diagnostic appointment produces the treatment plan. The treatment plan is the basis for the clinical decision. Remote quoting without imaging produces an estimate, not a plan. The diagnostic appointment is when the decision is made, not before. |
| "Any dentist can do full-mouth rehabilitation." | FMR is a prosthodontic and interdisciplinary procedure. General dentists with additional training may manage simple cases. Complex cases, full-arch implants, zygomatic implants, combined orthodontic and restorative rehabilitation, require specialist-led teams. Ask for the qualifications, not just the credentials. |
| "Tooth-supported rehabilitation is always better than implants." | Each modality has indications. If the tooth cannot be preserved, structurally, periodontally, or endodontically, extracting it and placing an implant in a healthy socket produces a more predictable outcome than attempting to restore a compromised tooth. |
Curious about costs and timelines?

People Also Ask
How long does full-mouth rehabilitation take?
Air travel after implant surgery is typically safe 24–48 hours post-procedure for most patients. The surgical protocol at Stunning Dentistry is structured so that the healing trajectory is stable and predictable before departure. Patients leave with written postoperative instructions, emergency contact details, and a defined protocol for managing common postoperative concerns while in transit and after return.
Want a personalised treatment plan?
Ask Your Doctor
Bring these questions to your consultation. They reveal clinical quality and expose gaps in the treatment plan.
1. Which diagnostic framework governs the occlusal design of my case, and how is my jaw position captured and confirmed before any tooth is prepared or any implant is placed?
2. What imaging have you reviewed, and can you show me the CBCT analysis that supports the implant plan, specifically the bone volume, bone quality, and distance from nerve or sinus?
3. Will there be a provisional phase? For how long will I wear the provisional before the definitive restoration is fabricated?
4. What is your protocol if an implant fails, before osseointegration, and after osseointegration?
5. Who else is involved in my case, and what are their specific qualifications? Will I meet them before treatment begins?
6. What materials will be used for the definitive prosthetic, and can you show me the manufacturer documentation?
7. What does the warranty cover, what does it exclude, and how do I access warranty service if I am back in Canada?
8. What does the maintenance schedule look like after I return home, and which of those tasks can my Canadian dentist perform?
9. Are there any systemic health factors in my profile that could affect healing, and how do you propose to manage them?
10. What would make me a poor candidate for the modality you are recommending, and what would change the plan if that condition were present?
Questions about this procedure?
For Canadian Patients: Your Journey to India
What does the full-mouth rehabilitation process look like for Canadian patients travelling to India?
> Most Canadian patients complete the clinical work in a single 7–10-day visit to New Delhi: diagnostic evaluation, CBCT, treatment plan approval, implant surgery and immediate provisional, and discharge with written postoperative instructions and the first review appointment scheduled. The definitive prosthetic phase can be coordinated either by a return visit or, in tooth-supported cases, by completing definitives within the same initial visit.
For Canadian patients, the decision to pursue full-mouth rehabilitation abroad is almost always a cost decision initially, and a research decision subsequently. The cost differential between Stunning Dentistry and the Canadian private market is real, consistent, and large enough that the total out-of-pocket figure including flights and accommodation remains significantly lower than the Canadian treatment cost alone. But the decision should be made on clinical grounds, not on cost alone.
At Stunning Dentistry, the pre-travel process begins with a remote case review. You submit your existing dental records, X-rays, and a clinical photograph series. We review the records and provide a preliminary assessment of modality suitability and an indicative cost range in CAD. This review is not a treatment plan, it is a preliminary filter to determine whether an in-person diagnostic visit is indicated. Once you arrive, the full diagnostic protocol confirms the plan.
| Travel Phase | What Happens |
|---|---|
| Remote pre-assessment | Submit records, photographs, existing X-rays. Receive preliminary modality assessment and CAD indicative range. |
| Flight and arrival | Direct flights available from Toronto, Vancouver, Calgary, Montreal to New Delhi (Indira Gandhi International). Travel time: 14–16 hours. |
| Day 1: Diagnostic appointment | CBCT, RVG, intraoral scan, clinical examination, photographs, treatment plan presentation, patient approval |
| Day 2: Surgical preparation | Anaesthetic assessment, pre-surgical medication briefing, consent finalisation |
| Day 3–5: Surgical phase | Extractions (if indicated), implant placement, immediate provisional (if primary stability criteria met) |
| Day 6–7: Recovery and review | Post-surgical review, hygiene instruction, night guard fitting, discharge with written protocol |
| Return to Canada | Post-surgical RVG emailed to your Canadian dentist; written care protocol and emergency contact confirmed |
| Month 4–6: Definitive phase | Return visit for definitive prosthetic placement; or remote coordination if tooth-supported case |
Ready to discuss your options?
What This Costs in CAD: Your Out-of-Pocket Reality
What is the total out-of-pocket cost for a Canadian patient for full-mouth rehabilitation at Stunning Dentistry?
> A single-arch full-arch implant protocol costs CAD $10,000–$18,000 at Stunning Dentistry. Adding return flights (CAD $1,200–$2,000) and 10 days of accommodation (CAD $700–$1,500) gives a total of approximately CAD $12,000–$21,500, compared to CAD $50,000–$80,000 at a Canadian prosthodontist for the same protocol.
Figures are illustrative. Your actual cost is determined by your specific modality, bone situation, implant count, and material selection. The CAD indicative range is confirmed at the remote pre-assessment stage and finalised after the diagnostic appointment.
| Cost Item | Low Estimate (CAD) | High Estimate (CAD) |
|---|---|---|
| Full-arch implant protocol (single arch), Stunning Dentistry | $10,000 | $18,000 |
| Second arch (if bilateral) | $10,000 | $18,000 |
| Return flight (Toronto / Vancouver to New Delhi) | $1,200 | $2,000 |
| Accommodation (7–10 days, mid-range hotel near clinic) | $700 | $1,500 |
| Local transport (New Delhi airport to clinic, return) | $50 | $150 |
| Travel insurance (recommended, with pre-existing condition coverage) | $100 | $400 |
| **Total: single arch** | **~$12,050** | **~$22,050** |
| **Total: both arches** | **~$22,050** | **~$40,050** |
| **Canadian prosthodontist: single arch** | **$50,000** | **$80,000** |
| **Canadian prosthodontist: both arches** | **$100,000** | **$160,000** |
Curious about costs and timelines?
Is This Worth Flying For? The Decision Framework
Is it worth flying to India for full-mouth rehabilitation?
> For Canadian patients facing full-arch implant work costing CAD $50,000–$80,000 locally, the CAD $12,000–$22,000 total cost at Stunning Dentistry represents a difference large enough to absorb all travel costs with a substantial reserve. The clinical case for dental travel is strongest when: the procedure is complex and elective, the cost differential is significant, the receiving clinic operates to verifiable clinical standards, and aftercare can be managed locally.
The decision to travel for dental rehabilitation is not primarily a financial decision, it is a clinical trust decision. The cost differential only justifies the travel if the clinical outcome is equivalent. The questions worth asking are: Is this clinic operating to the same diagnostic standard as a Canadian specialist would? Are the materials, the implant systems, and the protocols equivalent? Is there a genuine warranty, with a documented fly-back clause, or is the warranty marketing language? Is there a 10-year open file, or does the relationship end at the airport?
At Stunning Dentistry, we do not pressure a timeline for the treatment decision. The remote pre-assessment is provided without obligation. The diagnostic appointment in New Delhi is the commitment point, and that commitment is to a clinical evaluation, not to a treatment contract. The treatment plan is presented after the diagnostic session, the patient approves each phase, and no irreversible procedure begins without the three-stage approval gate being confirmed.
| Factor | Favours Travelling | Favours Local Treatment |
|---|---|---|
| Procedure complexity | High, requires interdisciplinary team | Low, single-unit, manageable locally |
| Cost differential | Large (≥CAD $30,000 saving) | Small (marginal saving does not justify travel) |
| Clinic verification | Credentials and protocols verifiable | Cannot verify standards of receiving clinic |
| Medical profile | Stable; suitable for travel post-surgery | Active systemic condition requiring local monitoring |
| Aftercare access | Canadian dentist willing to support follow-up | No local dental support; poor access |
| Urgency | Elective, can plan and travel | Emergency, needs immediate local management |
Want a personalised treatment plan?
Pre-Travel Checklist for Canadian Patients
Before booking flights, confirm each of the following:
Clinical preparation
- [ ] Existing dental records and X-rays submitted for remote pre-assessment and reviewed
- [ ] Remote pre-assessment received: indicative modality confirmed, CAD range understood
- [ ] Diagnostic appointment booked (separate from treatment)
- [ ] GP liaison completed if you have diabetes, bisphosphonate use, anticoagulant therapy, or recent radiotherapy
- [ ] Current medications list prepared (generic and brand names)
- [ ] Allergy history documented (including anaesthetic allergies if known)
- [ ] Flights booked: direct or single-connection recommended
- [ ] Accommodation booked within reasonable distance of the clinic
- [ ] Travel insurance confirmed: pre-existing condition coverage included; medical evacuation coverage included
- [ ] Extended health benefits policy reviewed: implant coverage terms confirmed
Post-treatment preparation
- [ ] Canadian dentist briefed on planned treatment: willing to support follow-up maintenance
- [ ] Night guard discussed: whether it will be fitted in India or arranged locally on return
- [ ] 7–10-day diet restriction understood: soft diet post-surgery
- [ ] Emergency contact protocol confirmed with Stunning Dentistry: direct line and remote consultation access
- [ ] Return-visit timing discussed for definitive phase (if implant case)
Questions about this procedure?

Back in Canada: Your Follow-Up Plan
What follow-up care do Canadian patients need after returning home from full-mouth rehabilitation?
> On return to Canada, you need a local dentist or periodontist to perform 6-monthly hygiene appointments with implant-specific instruments, an annual radiographic bone-level check, and prosthetic screw torque verification. Stunning Dentistry provides a written aftercare protocol and maintains a 10-year open case file with remote consultation access for any questions or concerns between review appointments.
Returning home after implant surgery does not end the clinical relationship. The healing phase, the 4–6 months between implant placement and definitive restoration, requires local professional monitoring in Canada. The objective of that monitoring is early identification of peri-implant issues before they affect osseointegration, and management of any soft tissue healing concerns that arise during the healing period.
At Stunning Dentistry, we provide every patient with a printed and emailed clinical summary that includes the implant system used, the brand and lot number of each implant, the torque specifications for prosthetic screws, the definitive material specifications, and the prescribed hygiene protocol. This document travels with the patient and is designed to be handed directly to the Canadian dental team.
| Follow-Up Task | Frequency | Recommended Provider in Canada |
|---|---|---|
| Professional hygiene (titanium-safe instruments for implants) | Every 6 months | Dental hygienist or general dentist |
| Peri-implant probing and soft tissue assessment | Annually | General dentist or periodontist |
| Radiographic bone-level check | Annually (years 1–3); every 2 years thereafter | General dentist with periapical capability |
| Prosthetic screw torque verification | At 6 months and 12 months post-definitive | General dentist with implant driver kit (Stunning Dentistry provides torque specifications) |
| Night guard review | Annually or when signs of wear appear | General dentist |
| Stunning Dentistry review (video or in-person) | Year 1, 3, 5, 10 | Stunning Dentistry remote or in-person |
Ready to discuss your options?
If Something Goes Wrong After You Are Home
What happens if a complication occurs after I return to Canada?
> Contact Stunning Dentistry directly via the emergency communication line provided at discharge. Common early complications, swelling, mild bleeding, loose provisional screw, can be managed remotely with guidance and by your local dentist. If a problem is traceable to Stunning Dentistry's clinical work and is identified at a documented review appointment, the fly-back-eligible clause of the 10-year warranty applies.
Complications in implant and prosthetic rehabilitation occur. The relevant question is not whether complications are possible, they are, in any clinical context, but what the management protocol is when they occur. A clinic that provides a warranty without a documented complication management protocol is providing a document, not a service.
At Stunning Dentistry, every patient leaves with a direct emergency communication line, not a general enquiry address. The 10-year open file means that every piece of clinical information from the original treatment is available at each review appointment. If a year-10 review examination surfaces a finding that is traceable to Stunning Dentistry's clinical work, the fly-back eligibility clause of the warranty applies: we cover the return journey and the corrective procedure. The exclusions from the warranty are stated in writing: they include damage from trauma, damage from hygiene failure, and complications arising from conditions that were not disclosed at the diagnostic stage.
| Complication Type | First Step | Second Step |
|---|---|---|
| Swelling beyond Day 7 | Continue anti-inflammatory medication; photograph and send to Stunning Dentistry | If worsening, attend local emergency dental or hospital for assessment |
| Provisional screw loose | Contact local dentist for re-torquing; Stunning Dentistry will provide torque specification | If provisional not retained, attend local dentist urgently |
| Implant mobility (before definitive) | Attend local dental assessment same day; photograph; contact Stunning Dentistry | Remote assessment of radiographs; management plan coordinated |
| Peri-implant swelling (after osseointegration) | Attend local periodontist for assessment; radiograph | Remote review with Stunning Dentistry; management protocol issued |
| Prosthetic fracture | Attend local dentist for assessment; photograph the fracture | Remote consultation with Stunning Dentistry; repair or replacement protocol |
Curious about costs and timelines?

Your Dental Tourism Safety Framework
Use this framework to evaluate any clinic, including Stunning Dentistry, before committing to treatment abroad.
| Verification Item | What to Ask | What a Credible Clinic Provides |
|---|---|---|
| Lead clinician credentials | "Can I verify your prosthodontic qualifications and specialty body memberships?" | Full name, degree, issuing institution, and specialty body member IDs |
| Implant brand | "Which implant system do you use and can I see the manufacturer documentation?" | Brand name, system name, and certificate of authorised surgeon status |
| Sterilisation standard | "What sterilisation protocol do you use and how is it audited?" | Class B autoclave; batch logging; quarterly audit documentation |
| Diagnostic standard | "What imaging is included in the diagnostic phase?" | CBCT + RVG as minimum for implant cases |
| Warranty | "Can I see the full warranty document before I agree to treatment?" | Written document with named coverage, named exclusions, and duration |
| Post-treatment access | "How do I reach you if something goes wrong after I return home?" | Direct communication line, not a general contact form |
| Fly-back clause | "Under what conditions does fly-back coverage apply?" | Specific conditions stated in writing, not verbal promise |
| Canadian dentist liaison | "Will you provide clinical documentation for my Canadian dentist?" | Clinical summary with implant specifics, torque values, and hygiene protocol |
Want a personalised treatment plan?
Book a Clinical Evaluation
If you are uncertain whether full-mouth rehabilitation is indicated for your case, the appropriate next step is a diagnostic evaluation, not a treatment commitment.
Secondary CTA: Request Remote Case Review
Questions about this procedure?
Ready to discuss your options?
Curious about costs and timelines?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










