Full-Mouth RehabilitationRebuilding an Entire Dentition Through a Sequenced, Multi-Specialist Protocol
- Most patients who arrive on this page have already had a conversation that started with a sentence like: "I'm afraid the whole mouth is going to need rebuilding." A Toronto prosthodontist has pointed at a CBCT and traced the pattern of wear.
An Edmonton oral surgeon has explained why the remaining implants cannot be saved.

Full-Arch Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Immediate Load
Full-arch or multiple implant cases where provisional teeth are placed shortly after surgery in suitable clinical conditions.

Multiple Implant Rehabilitation
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.

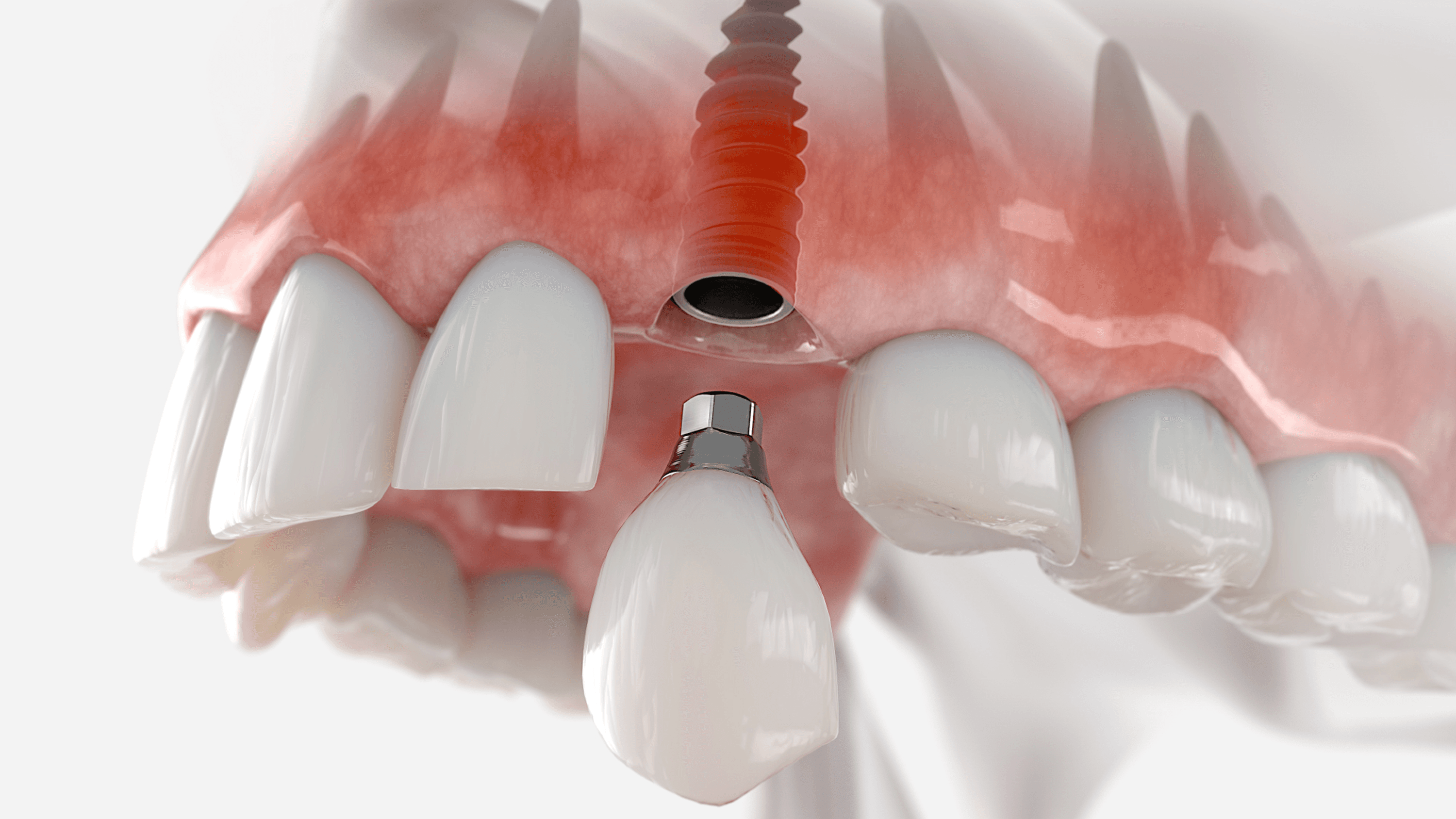
Single Tooth Implant
Single-tooth replacement with an implant and crown for a natural-looking, long-lasting result.

Bone Grafting & Advanced Surgical Support
Regenerative procedures performed to establish adequate bone volume for stable implant placement.

Revision & Complex Implant Cases
Complete upper or lower arch reconstruction using strategically placed implants to restore full function and structure.
Overview
Most patients who arrive on this page have already had a conversation that started with a sentence like: *"I'm afraid the whole mouth is going to need rebuilding."* A Toronto prosthodontist has pointed at a CBCT and traced the pattern of wear. An Edmonton oral surgeon has explained why the remaining implants cannot be saved. A Vancouver periodontist has put a number on the bone loss. The patient has been given a cost figure that makes the conversation feel like it belongs to someone else's life. Then they begin searching.
At Stunning Dentistry, full-mouth rehabilitation is managed under protocol SD-FMR-05: dual-clinician sign-off between Dr. Priyank Sethi and a senior prosthodontist before any irreversible treatment begins. No implant is placed, no tooth is prepared, no prosthetic is seated without that diagnostic gate being confirmed and documented. Every case that enters the SD-FMR-05 pathway is treated as a long-term clinical commitment, not a transaction.
| What This Article Covers | Why It Matters |
|---|---|
| The diagnostic frameworks that govern case planning | Without a named framework, there is no plan, only a series of procedures |
| The five modalities and how the choice is made | Modality selection errors are the primary driver of retreatment |
| The step-by-step process at Stunning Dentistry | Understanding the sequence reduces fear and improves patient cooperation |
| The evidence base for outcomes at 5 and 10 years | Confidence should come from published data, not clinic claims |
| The Canada-specific cost and logistics reality | The financial decision cannot be made without accurate comparators |
Questions about this procedure?
What Is Full-Mouth Rehabilitation?
What is full-mouth rehabilitation in clinical terms?
> Full-mouth rehabilitation is the simultaneous or staged reconstruction of every functional tooth surface across one or both dental arches. It addresses structure, occlusion, function, and aesthetics as one coordinated clinical plan. Depending on the case, it involves implants, crowns, bone grafting, periodontal treatment, endodontics, and smile design, executed by an interdisciplinary team in a defined sequence.
Full-mouth rehabilitation is not a procedure. It is a diagnostic and treatment category that encompasses every modality available to reconstruct a compromised dentition: full-arch implant protocols, tooth-supported crown and veneer reconstruction, hybrid implant-plus-tooth cases, implant-retained overdentures, and staged orthodontic-plus-restorative pathways. The category is defined not by the techniques it uses but by the scope of the problem it addresses, the entire arch, simultaneously or in sequence.
At Stunning Dentistry, the first determination in every consultation is whether full-mouth rehabilitation is the appropriate category for this specific case. That determination is made from diagnostic evidence, CBCT, RVG, intraoral scans, mounted study models, and clinical photographs, not from the patient's chief complaint or their preference for a specific modality. The diagnostic appointment establishes the category before the plan is written.
| FMR Category | Clinical Starting Point | Typical Protocol |
|---|---|---|
| Full-arch implant | All or most teeth missing or non-restorable | All-on-4, All-on-6, zygomatic implants |
| Tooth-supported reconstruction | Teeth present but structurally compromised across multiple units | Full-arch crown and veneer preparation under Kois framework |
| Hybrid implant + tooth | Partial edentulism with intact restorable units | Sequenced: implants placed, tooth restorations after osseointegration |
| Implant-retained overdenture | Full arch; removable prosthetic preferred or indicated | 2–4 implants; definitive overdenture at 3–4 months |
| Staged orthodontic + restorative | Skeletal or occlusal misalignment affecting load distribution | Orthodontic correction first; restorative completion after |
Ready to discuss your options?

Why Full-Mouth Rehabilitation: The Clinical Case
Why is full-mouth rehabilitation recommended rather than treating individual teeth?
> When structural compromise spans multiple arch segments, treating individual teeth in isolation produces sequential failures rather than a stable outcome. Full-mouth rehabilitation addresses the biomechanical system, occlusal load distribution, bone support, and functional stability across the entire arch, as a single coordinated problem. Individual repairs in a compromised system each fail faster than the same repair in a stable one.
The clinical case for full-mouth rehabilitation over segmental or isolated restorative treatment rests on one biomechanical principle: the oral system functions as an integrated whole. When occlusal load is distributed correctly across a full complement of teeth in good structural health, each restoration carries a predictable share. When the system is compromised, by missing teeth, by collapsed vertical dimension, by bone loss, the remaining restorations carry disproportionate load. They fail faster. The patient returns. More is extracted. The cycle continues.
At Stunning Dentistry, we present both pathways to every patient whose complexity falls in the borderline zone: full-mouth rehabilitation now, or segmental management over time. We document the clinical rationale for each, the expected outcome of each, and the cost trajectory of each. The choice belongs to the patient, but the choice is made with accurate clinical information, not with the assumption that the conservative option is always the right one.
| Approach | Appropriate For | Risk in a Compromised Arch |
|---|---|---|
| Segmental / isolated restorative | Isolated problems in a structurally stable arch | Each new restoration in a compromised system carries disproportionate load, higher failure rate |
| Full-mouth rehabilitation | Multiple-segment compromise; failed prior restorations; collapsed occlusion | Higher upfront complexity; pays off in long-term stability and reduced retreatment |
| Phased full-mouth rehabilitation | Complex cases where all work cannot be completed in one visit | Acceptable when each phase leaves the system in a more stable state than it entered |
Curious about costs and timelines?
Diagnostic Frameworks That Govern the Rebuild
What diagnostic frameworks are used to plan full-mouth rehabilitation?
> The four principal frameworks are the Dawson Concept, the Kois Technique, the Pankey Philosophy, and the Hobo-Takayama Twin-Stage Technique. Each provides a structured protocol for capturing jaw position, analyzing occlusal risk, and sequencing the clinical work. The framework governs every decision from initial examination through definitive seating.
Full-mouth rehabilitation without a named diagnostic framework is a sequence of dental appointments without a clinical plan. The frameworks below are not theoretical preferences, they are structured decision systems with defined steps, peer-reviewed evidence bases, and international postgraduate training programmes. The framework selected governs how the prosthodontist establishes jaw position, designs the bite, sequences the phases, and tests the outcome before committing to the definitive restoration.
At Stunning Dentistry, every FMR case is governed by a named framework documented in the case record. For full-arch implant cases, the Dawson Concept governs centric relation capture and occlusal design. For tooth-supported cases, the Kois 6-step diagnostic framework structures the case from initial examination through provisional testing. The framework selection is made on case type and documented in the treatment plan disclosed to the patient before irreversible work begins.
| Framework | Primary Application | Core Principle |
|---|---|---|
| Dawson Concept | Full-arch implant and tooth-supported cases | Centric relation as the stable, reproducible mandibular position, all occlusal design proceeds from this position |
| Kois Technique | Tooth-supported and aesthetic-driven cases | 6-step protocol: periodontal, occlusal, structural, and biomechanical risk assessed sequentially |
| Pankey Philosophy | Balanced occlusion, phased treatment | Anterior guidance established first; posterior stops second, complexity built in defined stages |
| Hobo & Takayama | Long-span or high-complexity cases | Twin-stage technique: complete diagnostic phase and provisional testing before definitive commitment |
Want a personalised treatment plan?

Long-Term Survival Data
What does the long-term evidence say about full-mouth rehabilitation outcomes?
> Peer-reviewed cohort data supports full-mouth rehabilitation as durable and predictable when executed under interdisciplinary protocols. Implant survival rates for full-arch protocols (All-on-4, All-on-6) exceed 94% at 5 years in published studies. Tooth-supported FMR shows comparable durability when periodontal foundation is confirmed and a provisional testing phase precedes definitive fabrication.
The evidence base for full-mouth rehabilitation spans more than five decades of peer-reviewed clinical research. The volume, function, and longevity outcomes for implant-supported full-arch prosthetics are among the most studied topics in contemporary prosthodontic and implant literature. The evidence supports the procedure, what it does not support is execution outside a defined diagnostic and clinical standard.
At Stunning Dentistry, clinical decisions are referenced against the peer-reviewed literature in implantology, prosthodontics, and endodontics. We do not substitute internal outcome claims for published evidence. When we cite a survival rate, we cite the reference it comes from, and we explain what the study population was and how it compares to your case.
| Evidence Source | Journal | Key Metric |
|---|---|---|
| All-on-4 cohort data (Maló et al.) | Clinical Oral Implants Research | 94–99% implant survival at 5 years; bone loss <1.5mm at 5 years |
| Tooth-supported FMR outcomes | Journal of Prosthetic Dentistry | >90% restoration survival at 5 years with provisional testing phase |
| Zygomatic implant outcomes | Int J Oral Maxillofac Implants | 95–97% cumulative survival at 5 years; peri-implant sinusitis 5–10% |
| Periodontal-implant relationship | Journal of Periodontology | Pre-implant periodontal control reduces peri-implantitis incidence |
| Digital workflow accuracy | International Journal of Prosthodontics | Guided placement deviation ≤1.2mm apex; ≤4° angulation |
Questions about this procedure?
Clinical Equipment and Technology
What clinical technology is used in full-mouth rehabilitation today?
> Contemporary full-mouth rehabilitation uses intraoral scanning for digital impressions, CBCT for 3D bone mapping, CAD/CAM for prosthetic design, digital face bow and virtual articulator for bite simulation, and PMMA-milled provisionals for functional testing before any ceramic or zirconia definitive is fabricated and seated.
The digital workflow in full-mouth rehabilitation has materially changed how diagnostic data is captured, stored, and transmitted, and how provisional and definitive restorations are designed and fabricated. The transition has not changed the diagnostic framework. The Dawson Concept applied with a digital face bow and virtual articulator produces the same information as the same concept applied with an analog face bow and a mechanical articulator, but with higher precision, less chair time, and lower laboratory error rates.
At Stunning Dentistry, the digital workflow includes intraoral scanning (Trios 4 / Medit i700), CBCT-based implant planning (coDiagnostiX), CAD/CAM design for provisional and definitive restorations (3Shape / exocad), and virtual articulator simulation before irreversible preparation begins. PMMA-milled provisionals are fabricated for every full-arch case and worn for a minimum of 4–6 weeks before the definitive design is approved for fabrication.
| Digital Tool | Purpose | Stage in FMR |
|---|---|---|
| Intraoral Scanner (Trios 4 / Medit) | Full-arch digital impression; bite registration | Diagnostic and restorative phases |
| CBCT (Planmeca / Carestream) | Bone volume, sinus, nerve mapping, implant site analysis | Diagnostic phase |
| Implant Planning Software (coDiagnostiX) | Surgical guide design; virtual implant placement | Pre-surgical phase |
| Digital Face Bow / Virtual Articulator | Condylar pathway; excursive movement simulation | Diagnostic and provisional phase |
| CAD/CAM (3Shape / exocad) | Prosthetic design: crowns, bridges, full-arch prosthetics | Laboratory phase |
| PMMA Milling | Functional provisional fabrication and testing | Provisional phase |
Ready to discuss your options?
Symptoms and Signs That Indicate Candidacy
What symptoms indicate that full-mouth rehabilitation may be needed?
> Key clinical indicators include: significant tooth wear that has shortened teeth or collapsed the bite; multiple loose, fractured, or missing teeth across both arches; jaw pain or clicking associated with a changing bite; inability to chew on both sides; multiple failed crowns or bridges; and a previous assessment stating that individual tooth repair is no longer viable across multiple sites.
Full-mouth rehabilitation is indicated by specific clinical findings, not by symptom severity alone. Pain does not indicate FMR. Pain is a symptom; FMR is indicated by the structural and functional findings that cause or accompany the pain. A patient in significant discomfort from a single infected tooth needs endodontic treatment or extraction, not full-mouth rehabilitation. The distinction matters because the two categories differ in complexity, cost, and timeline by an order of magnitude.
At Stunning Dentistry, candidacy is established from diagnostic evidence, not from the patient's report of symptoms. The diagnostic appointment produces a written findings summary with the imaging referenced, the clinical measurements recorded, and the modality rationale explained. That document is the basis of the treatment plan. No plan is presented without it.
| Indication | What the Clinician Observes | What It Means for Treatment |
|---|---|---|
| Severe occlusal attrition | Shortened teeth; lost vertical dimension; flat occlusal surfaces | Tooth-supported or implant-supported FMR depending on remaining tooth viability |
| Advanced periodontitis | Bone loss >50% on multiple teeth; mobility; deep probing depths | Extractions + bone augmentation + implant-supported |
| Multiple failed restorations | Fractured crowns; failed bridges; recurrent decay beneath large restorations | Diagnostic reassessment; hybrid or full-arch depending on remaining teeth |
| Developmental defects | Discoloured, soft, or poorly formed enamel and dentine | Case-specific; tooth-supported if structure allows |
| Post-traumatic destruction | Multiple teeth fractured or avulsed from injury | Implant or tooth-supported; urgent triage first |
| Failed prior rehabilitation | Failed implants; failed bridges; failed denture with bone loss | Salvage assessment; revised modality selection |
Curious about costs and timelines?

Benefits of Full-Mouth Rehabilitation
What are the documented benefits of full-mouth rehabilitation?
> Documented benefits include restored masticatory function across the full arch, re-established occlusal stability and vertical dimension, elimination of pain caused by structural collapse or muscle dysfunction, aesthetic restoration of the smile, and improved phonetics where tooth loss had altered speech. Long-term psychological quality-of-life improvements are documented in peer-reviewed patient satisfaction literature.
Full-mouth rehabilitation restores function before it restores aesthetics, and when it is properly planned, the functional outcome is the precondition for the aesthetic one. The rebuild of the occlusal system, the vertical dimension, the anterior guidance, the posterior load distribution, is what determines how long the aesthetic outcome will last. Crowns and veneers placed on a correctly designed occlusal foundation outlast the same restorations placed without one by a margin that is documented in the long-term prosthodontic literature.
At Stunning Dentistry, we document the functional outcome of the provisional phase before we commit to the definitive design. The patient must confirm that the new vertical dimension is comfortable, that the anterior guidance feels correct in function and in lateral movement, and that the aesthetic outcome of the provisional, the tooth size, shade, and proportion, reflects what they want before the definitive is fabricated. This gate prevents the most common cause of patient dissatisfaction in FMR: restorations that the patient approved in theory but had not tested in function.
| Benefit Category | What Is Restored | Timeline |
|---|---|---|
| Masticatory function | Full bilateral chewing efficiency | Provisional phase: immediate; definitive: months 4–6 |
| Occlusal stability | Vertical dimension; centric stops; anterior guidance | Established and tested during provisional phase |
| Aesthetic outcome | Tooth shade, form, proportion, smile architecture | Designed in provisional; finalised at definitive |
| Phonetics | Speech affected by tooth loss or collapsed bite | Restored with provisional; refined at definitive |
| Pain resolution | TMJ pain, muscle fatigue from collapsed VDO | Resolves as correct VDO is established and maintained |
| Psychological | Self-confidence; social comfort; quality of life | Reported at 6-month and 1-year follow-up |
Want a personalised treatment plan?

Recovery and Phasing Timeline: Month 0 to Year 1
How long does recovery from full-mouth rehabilitation take?
> For full-arch implant cases, the surgical recovery period is 5–7 days of significant swelling and moderate discomfort, managed with anti-inflammatory and analgesic medication. Patients are eating soft foods within 48 hours and living normally within 7–10 days. The full osseointegration period runs 4–6 months. Tooth-supported cases have no surgical recovery, preparation appointments are managed with local anaesthesia.
For tooth-supported cases, the timeline compresses to two visits: preparation and provisional placement (Day 1–2), then definitive seating 4–6 weeks later after laboratory fabrication.
| Month | What Is Happening Clinically | Patient Experience |
|---|---|---|
| Month 0: Surgery | Extractions + implant placement + immediate provisional seated same day | Swelling, pressure, mild-to-moderate soreness for 48–72 hours; managed with medication |
| Week 1–2 | Soft tissue healing; provisional in function; soft diet | Eating soft foods; normal speech; some fatigue |
| Month 1 | Early osseointegration; provisional testing phase begins | Normal diet restrictions easing; provisional adjusted if needed |
| Month 2–3 | Osseointegration progressing; provisional worn in full function | Normal function; provisional tested across all excursive movements |
| Month 4 | Osseointegration confirmation (clinical + radiographic) | Return appointment: scans for definitive fabrication |
| Month 4–6 | Laboratory fabrication of definitive zirconia or ceramic prosthetic | Patient not in clinic during this period |
| Month 5–6 | Definitive seating; torque verification; final adjustments | Final prosthetic in place; warranty issued |
| Month 9–12 | First follow-up review | Radiographic bone level check; prosthetic review; hygiene assessment |
Questions about this procedure?
Complications and How They Are Managed
What complications can occur in full-mouth rehabilitation and how are they managed?
> The most common complications are: provisional screw loosening (managed by re-torquing at any dental office), peri-implant soft tissue irritation (managed with hygiene protocol adjustment), and extended swelling beyond 7 days (managed with continued anti-inflammatory medication and clinical assessment). Implant failure before osseointegration occurs in approximately 1–5% of cases and requires replacement at a defined healing interval.
Complications in implant and prosthetic rehabilitation occur. The relevant clinical question is not whether complications are possible, they are, in any context, but what the management protocol is when they occur, how rapidly the clinic responds, and what the patient's recourse is. A clinic that does not discuss complications before treatment is not a clinic that has eliminated them. It is a clinic that has not disclosed them.
At Stunning Dentistry, every patient receives a written complication management protocol at discharge. The protocol documents the most common early complications, the first response for each, when to contact Stunning Dentistry directly, and when to attend local emergency dental care. A direct emergency communication line, not a general contact form, is provided to every patient. The 10-year open case file means that any complication that surfaces at a review appointment is managed with full access to the original diagnostic and surgical record.
| Complication | Timing | Incidence | Management |
|---|---|---|---|
| Provisional screw loosening | Any time post-surgery | Common | Re-torque at any dental office with implant driver; Stunning Dentistry provides torque specification |
| Soft tissue irritation at provisional flange | Weeks 1–4 | Common | Provisional flange adjustment; hygiene protocol modification |
| Swelling beyond Day 7 | Week 1–2 | Occasional | Continue anti-inflammatory; clinical assessment if worsening |
| Early implant failure (pre-osseointegration) | Month 1–4 | 1–5% of implants | Implant removal; site healing; replacement at 3–4 months |
| Peri-implantitis (post-osseointegration) | Year 1 onward | Hygiene-dependent | Debridement first; surgical intervention if progressive; implant removal if critical |
| Ceramic/zirconia fracture | After definitive seating | Uncommon | Repair or replacement; covered under warranty for material defects |
Ready to discuss your options?

Full-Mouth Rehabilitation vs Segmental Restorative Dentistry
When should a patient choose full-mouth rehabilitation over treating individual teeth?
> Full-mouth rehabilitation is indicated when structural compromise spans multiple arch segments and cannot be resolved by targeted single-unit treatment. If three or more adjacent teeth have failed or are failing in the context of a compromised occlusal system, segmental restorative treatment addresses components of a problem whose cause is system-wide. Full-mouth rehabilitation addresses the cause.
Segmental restorative dentistry, treating one quadrant, one tooth, one failed crown at a time, is the correct approach for patients whose dental problems are isolated to specific sites within an otherwise stable and healthy arch. For that category of patient, full-mouth rehabilitation would be clinical overtreatment. The challenge is that the category of patient with truly isolated dental problems and a stable arch is not the category that typically arrives asking about full-mouth rehabilitation.
At Stunning Dentistry, we present the choice explicitly for every borderline case. The treatment plan document we provide to patients in the moderate-complexity zone includes both pathways: full-mouth rehabilitation now with the clinical rationale and 5-year cost projection, and segmental management over time with the same information. The patient makes the decision with complete data.
| Factor | Segmental Restorative | Full-Mouth Rehabilitation |
|---|---|---|
| Appropriate when | Isolated failure in a stable arch | Multiple-segment compromise; compromised occlusal system |
| Cost trajectory | Lower upfront; higher cumulative if problem is progressive | Higher upfront; lower cumulative retreatment in a stable system |
| Timeline | One tooth at a time; years of sequential treatment | Defined phases; 4–7 months from diagnosis to definitive |
| Risk in wrong case | Progressive failure continues; increasing cost and tooth loss | Overtreatment of an isolated problem |
| Decision basis | Clinical findings, not patient preference | Clinical findings, not patient preference |
Curious about costs and timelines?
FMR Modality Comparison: Tooth-Supported, Implant-Supported, Hybrid
How do the main full-mouth rehabilitation modalities compare to each other?
> The three main categories are tooth-supported reconstruction (crowns and veneers on retained teeth), implant-supported fixed prosthetics (All-on-4, All-on-6, zygomatic), and hybrid cases combining both. The choice is made on remaining tooth viability, bone volume, surgical risk, and the patient's systemic health, not on patient preference for implants or preference for avoiding surgery.
Modality is not chosen by the patient, it is determined by the diagnostic examination. A patient who prefers implants but has retained teeth with viable roots and controlled periodontium is not a full-arch implant candidate. A patient who prefers to keep their teeth but has roots with bone loss beyond 60% on most units is not a tooth-supported candidate. The examination determines the modality. The plan follows from the examination.
| Factor | Tooth-Supported | Implant-Supported (Full-Arch Fixed) | Hybrid (Implant + Tooth) |
|---|---|---|---|
| Requires surgery | No | Yes | Yes (partial) |
| Bone requirement | None | Moderate to high | Moderate |
| Remaining teeth used | All retained teeth | Not applicable | Retained teeth supplemented by implants |
| Reversibility | Partial (crowns removable) | No | No |
| Typical cost (Stunning Dentistry CAD) | Case-specific | $10,000–$18,000 per arch | Case-specific |
| Typical cost (Canadian prosthodontist CAD) | $25,000–$60,000 | $50,000–$80,000 per arch | $35,000–$70,000 |
| Timeline | 7–10 days + 4–6 weeks for definitives | 7–10 days + 4–6 months for definitives | Sequenced: 2 visits |
| Maintenance | 6-monthly hygiene; no implant-specific maintenance | Annual implant review; radiographic bone checks | Combination |
| Primary indication | Viable roots; controlled periodontium | Non-restorable teeth; insufficient bone for natural roots | Mixed: some sites viable, some require implants |
Want a personalised treatment plan?

What Determines the Cost of Full-Mouth Rehabilitation?
What factors determine the cost of full-mouth rehabilitation?
> Cost is determined by: number of arches treated, number of implants, whether bone augmentation is required, implant brand tier, prosthetic material selected, duration of the provisional phase, and the number of specialist disciplines involved. A single-arch All-on-4 with standard bone volume costs significantly less than a bilateral zygomatic case with extended provisional testing.
These factors are assessed at the diagnostic appointment. The cost quoted before a diagnostic appointment with imaging is an estimate. The treatment plan produced after the diagnostic appointment is the actual cost, itemised by component, not presented as a single bundled figure.
| Cost Factor | Lower Cost | Higher Cost |
|---|---|---|
| Number of arches | Single arch | Both arches |
| Implant count | 4 implants (All-on-4) | 6–8 implants or zygomatic |
| Bone augmentation | None required | Sinus lift or major block graft |
| Implant brand | Osstem | Straumann SLActive or Nobel Biocare Active |
| Prosthetic material | PMMA long-term temporary | Monolithic zirconia or titanium-framed ceramic |
| Provisional phase | 4–6 weeks | 6–12 months (complex VDO changes) |
| Specialist involvement | Single-arch, standard anatomy | Multi-specialist: oral surgery + perio + endo + prosthodontics |
Questions about this procedure?
Step-by-Step: How Full-Mouth Rehabilitation Is Performed at Stunning Dentistry
What does the full-mouth rehabilitation process look like step by step?
> The process runs through three gates: diagnostic, surgical and provisional, and definitive. No gate opens before the previous one is completed and the patient has given documented approval. The diagnostic gate takes 1–2 days. The surgical and provisional gate takes 3–7 days. The definitive gate occurs 4–6 months later after osseointegration is confirmed.
Full-mouth rehabilitation at Stunning Dentistry does not begin with surgery. It begins with a diagnostic phase that determines what the surgery should accomplish, and whether surgery is indicated at all. The three-gate structure ensures that no irreversible procedure is taken without documented clinical rationale and documented patient consent.
The Journal of Prosthetic Dentistry and the clinical guidelines of the American Academy of Prosthodontics both identify patient-informed, staged consent as a standard of care for complex oral rehabilitation. The three-gate model at Stunning Dentistry operationalises that standard: each gate requires the patient to review, ask questions, and sign before the next phase begins.
If a clinic presents you with a treatment plan and a booking deposit in the same appointment, particularly before any imaging, you should treat that as a significant departure from clinical standard. The diagnostic appointment is when the plan is made. The booking is what happens after the plan is understood and accepted. These are different events and they should not happen simultaneously.
Gate 1, Diagnostic Phase (Day 1–2)
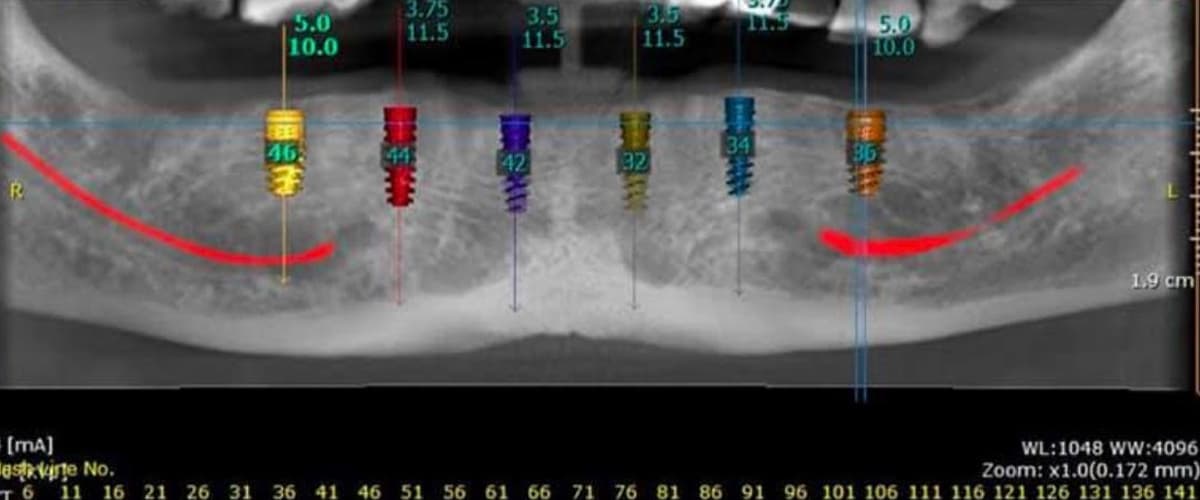
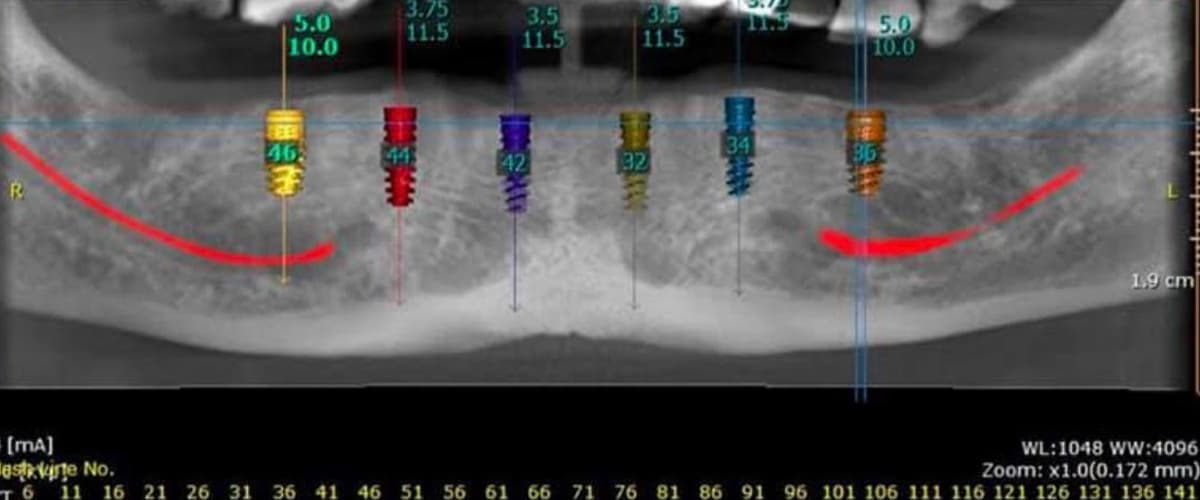
1. CBCT scan for bone volume, sinus anatomy, nerve proximity, and implant site analysis
2. RVG (periapical radiographs) for endodontic and periodontal status of retained teeth
3. Intraoral scanning: full-arch digital impression and occlusal registration
4. Clinical photography: facial, profile, retracted, and bite views
5. Periodontal charting: probing depths, mobility, furcation involvement
6. TMJ and occlusal assessment: condylar position, range of motion, signs of dysfunction
7. Diagnostic wax-up or digital mock-up: proposed prosthetic outcome
8. Three-stage patient approval: diagnostic findings → treatment plan → informed consent for each irreversible phase
Gate 2, Surgical and Provisional Phase (Day 3–7)
9. Extractions of non-restorable teeth under local anaesthesia; sedation available
10. Implant placement under protocol SD-FMR-05: dual-clinician sign-off before incision
11. Immediate loading: full-arch PMMA provisional fixed prosthetic placed same day if primary stability criteria are met
12. Post-surgical RVG for implant position confirmation
13. Discharge: soft diet protocol, oral hygiene instruction, night guard fitting if bruxism
Gate 3, Definitive Phase (Month 4–6 post-implant)
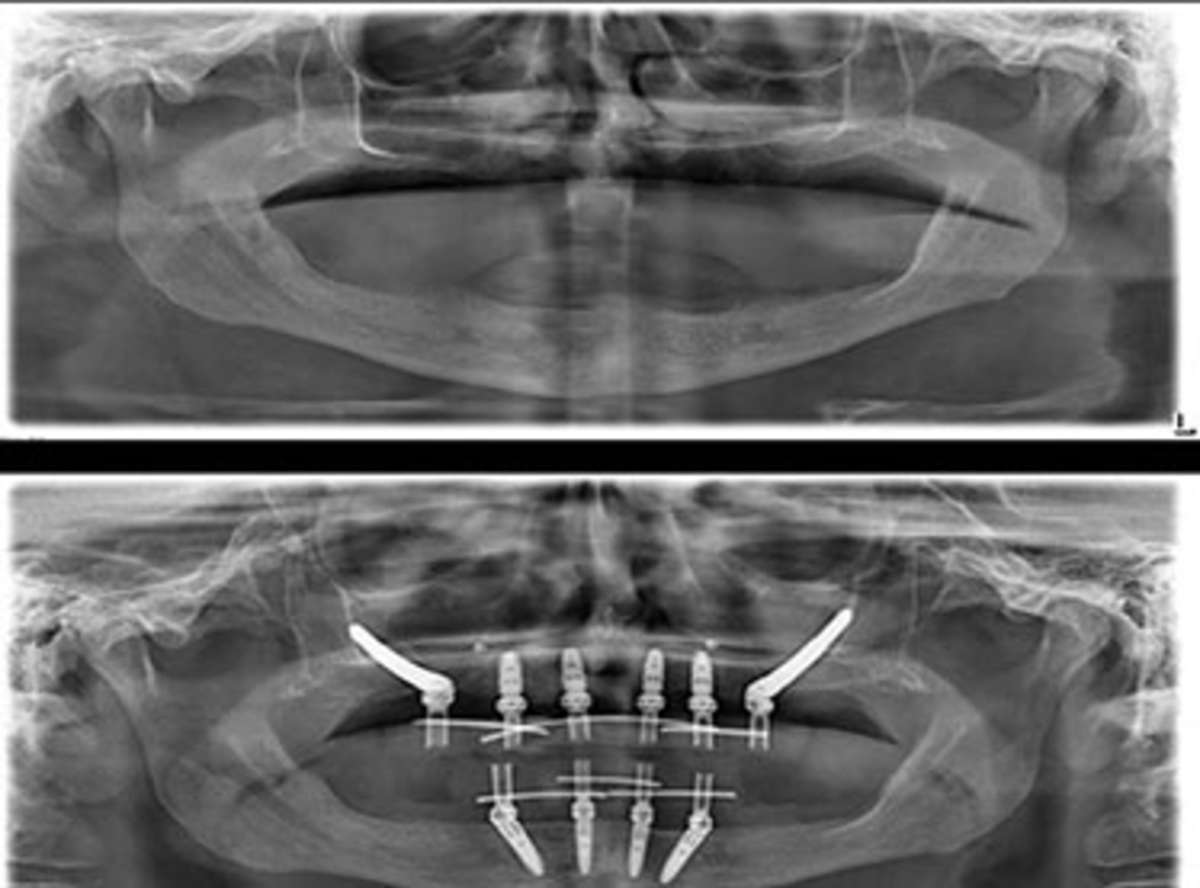
14. Osseointegration confirmed by clinical examination and radiographic bone-level assessment
15. Definitive impressions or intraoral scans for final prosthetic fabrication
16. Laboratory fabrication: monolithic zirconia, lithium disilicate, or titanium-ceramic framework
17. Definitive seating: torque verification, occlusal adjustment, aesthetic confirmation, documentation
18. 10-year written warranty issued; review schedule confirmed at Year 1, 3, 5, 10
| Gate | Days | What Happens |
|---|---|---|
| Diagnostic | Day 1–2 | Imaging, examination, mock-up, patient approval |
| Surgical + Provisional | Day 3–7 | Extractions, implant placement, immediate provisional |
| Definitive | Month 4–6 | Final scans, laboratory fabrication, definitive seating |
| Warranty issued | At definitive seating | 10-year written warranty; review schedule |
Ready to discuss your options?
Aftercare and Long-Term Maintenance
What maintenance does full-mouth rehabilitation require after treatment?
> Implant-supported cases require annual professional maintenance: peri-implant tissue assessment, radiographic bone-level check, prosthetic screw torque verification, and hygiene cleaning with implant-specific instruments. Tooth-supported cases require 6-monthly professional hygiene. All cases with bruxism require a night guard. The 10-year warranty covers clinical work, it does not replace home care or professional maintenance.
Osseointegration is a biological process, not a guarantee. Once the implant is in place and the prosthetic is seated, the long-term outcome depends on variables the clinic cannot control after the patient returns home: bone health, systemic health trajectory, oral hygiene, and maintenance compliance. Peri-implantitis, inflammation around the implant driven by biofilm accumulation, is the primary late complication of implant-supported rehabilitation. It is preventable. It is not self-limiting once established.
At Stunning Dentistry, every patient leaves with a printed and emailed clinical summary: implant system, brand, lot number of each implant, prosthetic screw torque specifications, prescribed home hygiene protocol, and the maintenance schedule. This document is designed to be handed directly to the Canadian dental team managing the patient's local follow-up. The Stunning Dentistry 10-year open file is available at every review appointment.
| Maintenance Task | Frequency | Provider |
|---|---|---|
| Professional hygiene (implant-safe instruments) | Every 6 months | Local Canadian hygienist / dentist |
| Peri-implant tissue and probing assessment | Annually | Local Canadian dentist or periodontist |
| Radiographic bone-level check | Annually (years 1–3); every 2 years thereafter | Local Canadian dentist |
| Prosthetic screw torque verification | 6 and 12 months post-definitive; then as indicated | Local Canadian dentist with implant driver kit |
| Night guard review | When signs of wear appear | Local Canadian dentist |
| Stunning Dentistry review (video or in-person) | Year 1, 3, 5, 10 | Stunning Dentistry |
Curious about costs and timelines?

Aftercare Responsibility Split: What You Do, What We Do
| Responsibility | Patient | Stunning Dentistry |
|---|---|---|
| Daily home hygiene | Brushing around implants with soft brush and interproximal brushes; water flosser recommended | Provide written protocol at discharge |
| Professional hygiene maintenance | Book and attend every 6 months with Canadian hygienist | Provide clinical summary for local team; advise on implant-specific instrument requirements |
| Annual radiographic review | Attend annual X-ray review with local Canadian dentist | Review radiographs remotely if uploaded to patient portal |
| Night guard | Wear nightly if bruxism; replace when worn | Fit initial night guard; advise on replacement indicators |
| Systemics management | Manage diabetes, smoking, medications, advise Stunning Dentistry of any changes | Adjust maintenance schedule if systemic risk profile changes |
| Implant-site concerns | Contact Stunning Dentistry immediately if swelling, mobility, or pain around implants | Respond within 24 hours; coordinate with local dentist as needed |
| Scheduled reviews | Attend Year 1, 3, 5, 10 review appointments | Maintain open case file; conduct review; document findings |
| Warranty claims | Contact Stunning Dentistry; attend review appointment | Assess claim; apply warranty terms as documented in written warranty |
Want a personalised treatment plan?

Myths vs Clinical Reality
| Myth | Clinical Reality |
|---|---|
| "Dental implants last a lifetime." | Implants can last for decades with correct maintenance. They are not unconditional lifetime biological structures. Peri-implantitis, prosthetic wear, and bone changes can affect them over time. |
| "Getting dental work done in India is risky." | Risk is determined by clinical protocols, diagnostic standards, sterilisation practices, and clinical team experience, not by geography. A clinic operating to international standards in New Delhi is not less safe than a clinic ignoring standards in Toronto. |
| "Full-mouth rehabilitation is just for cosmetic patients." | FMR is indicated by structural, functional, and periodontal criteria. Many patients pursue it because they cannot eat normally or because sequential repair has failed, not because of appearance dissatisfaction. |
| "The provisional is just a temporary measure." | The provisional is a functional prototype. It tests the new VDO, the anterior guidance, and the occlusal scheme before definitive fabrication. Cases where the provisional phase is skipped show higher rates of definitive restoration failure. |
| "One dentist can do all of this." | Complex FMR requires interdisciplinary management. No single clinician has equivalent specialty-level expertise across implant surgery, prosthodontics, periodontics, and endodontics simultaneously. |
| "The cheaper price means cheaper implants." | Implant material cost is a fraction of total treatment cost. Straumann and Nobel Biocare implants are available at the same wholesale cost in India as in Canada. The price differential reflects specialist labour, overhead, and insurance cost differences, not material differences. |
| "If something goes wrong, I'll be on my own." | Stunning Dentistry provides a direct emergency communication line, a 10-year open case file, remote consultation, and a written warranty with a fly-back-eligible clause for complications traceable to clinical work. |
| "Tooth-supported rehabilitation is always safer than implants." | Safety and appropriateness are case-dependent. Attempting to restore teeth with insufficient structural or periodontal viability produces more retreatment than placing an implant in a healthy socket after a timely extraction. |
Questions about this procedure?
People Also Ask
How long does full-mouth rehabilitation take for a Canadian patient travelling to India?
Dr. Priyank Sethi's MDS Prosthodontics and PhD credentials are verifiable through the issuing institutions. AAID and AACD memberships are verifiable through those organisations' member directories. Straumann and Nobel Biocare surgeon certifications are verifiable through those companies' certified surgeon directories. Ask for specific credential references, not brochure language.
Ready to discuss your options?

Ask Your Doctor
Bring these questions to any consultation. They distinguish clinics that plan from clinics that quote.
1. Which diagnostic framework governs the occlusal design of my case, and how do you capture and confirm jaw position before any irreversible procedure begins?
2. What imaging have you reviewed, and can you show me the CBCT analysis that supports the implant plan, bone volume, bone quality, and proximity to the nerve or sinus?
3. Will there be a provisional phase? For how long will I wear the provisional before the definitive is fabricated?
4. What is your protocol if an implant fails, before osseointegration, and after osseointegration?
5. Who else is involved in my case, and what are their specific qualifications? Will I meet them before treatment begins?
6. What materials will be used, implant brand, prosthetic material, framework type, and can you show me the manufacturer documentation?
7. What does the warranty cover, what does it exclude, and how do I access it if I am back in Canada?
8. What does the maintenance schedule look like, and which tasks can my Canadian dentist perform locally?
9. Are there systemic health factors in my profile that could affect healing, and how do you propose to manage them?
10. What would make me a poor candidate for the modality you are recommending, and what would change the plan?
Curious about costs and timelines?
For Canadian Patients: Your Journey to India
What does the process look like for a Canadian patient travelling to Stunning Dentistry for full-mouth rehabilitation?
> The process begins with a remote pre-assessment: submit existing records and photographs for a preliminary modality assessment and an indicative CAD cost range. The clinical visit to New Delhi takes 7–10 days covering the diagnostic appointment, surgery, provisional placement, and discharge. The definitive phase occurs 4–6 months later, either on a return visit or remotely coordinated for tooth-supported cases.
For Canadian patients, the decision to pursue full-mouth rehabilitation abroad typically begins with the cost figure from a local prosthodontist and ends with a research process that produces more questions than it answers. The question that matters most is not "is it cheaper?", the answer to that is yes, by a margin that makes the travel cost irrelevant. The question that matters is: "is the clinical outcome equivalent to what I would receive in Canada?"
At Stunning Dentistry, the pre-travel process begins with a remote case review. Submit your existing dental records, X-rays, and a clinical photograph series. We provide a preliminary assessment of modality suitability and an indicative CAD cost range. This is not a treatment plan, it is a preliminary filter. The treatment plan is produced at the diagnostic appointment in New Delhi after imaging and examination confirm the clinical findings.
| Stage | What Happens | Where |
|---|---|---|
| Remote pre-assessment | Records review; preliminary modality assessment; indicative CAD range | Remote (email / video) |
| Travel | Direct or single-connection flight to New Delhi Indira Gandhi International | From Toronto, Vancouver, Calgary, Montreal |
| Day 1–2: Diagnostic | CBCT, RVG, intraoral scan, exam, mock-up, treatment plan, patient approval | Stunning Dentistry, New Delhi |
| Day 3–5: Surgical | Extractions (if indicated), implant placement, immediate provisional | Stunning Dentistry, New Delhi |
| Day 6–7: Discharge | Post-surgical review, hygiene instruction, written protocol, emergency contact | Stunning Dentistry, New Delhi |
| Return to Canada | Clinical summary for Canadian dentist; remote check-in at 2 weeks | Remote |
| Month 4–6: Definitive | Return visit for definitive placement; or remote coordination for tooth-supported cases | Stunning Dentistry or remote |
Want a personalised treatment plan?
What This Costs in CAD: Your Out-of-Pocket Reality
What is the total cost for a Canadian patient for full-mouth rehabilitation at Stunning Dentistry including travel?
> A single-arch full-arch implant protocol costs CAD $10,000–$18,000 at Stunning Dentistry. Adding return flights (CAD $1,200–$2,000) and 10 days of accommodation (CAD $700–$1,500) gives a total of approximately CAD $12,000–$21,500, compared to CAD $50,000–$80,000 for the same protocol at a Canadian prosthodontist.
Figures are illustrative. Your actual cost is confirmed at the remote pre-assessment stage and finalised after the diagnostic appointment. CAD pricing is confirmed in writing before any treatment begins.
| Item | Low (CAD) | High (CAD) |
|---|---|---|
| Full-arch implant protocol, single arch (Stunning Dentistry) | $10,000 | $18,000 |
| Second arch (if bilateral) | $10,000 | $18,000 |
| Return flight (Toronto / Vancouver / Calgary to New Delhi) | $1,200 | $2,000 |
| Accommodation (7–10 days, mid-range near clinic) | $700 | $1,500 |
| Local transport (airport to clinic, return) | $50 | $150 |
| Travel insurance (recommended; pre-existing condition coverage) | $100 | $400 |
| **Total, single arch** | **~$12,050** | **~$22,050** |
| **Total, both arches** | **~$22,050** | **~$40,050** |
| **Canadian prosthodontist, single arch** | **$50,000** | **$80,000** |
| **Canadian prosthodontist, both arches** | **$100,000** | **$160,000** |
Questions about this procedure?
Is This Worth Flying For? The Decision Framework
Is it worth travelling to India for full-mouth rehabilitation as a Canadian patient?
> For Canadian patients facing full-arch implant work at CAD $50,000–$80,000 locally, the total Stunning Dentistry cost of CAD $12,000–$22,000 represents a difference that absorbs all travel costs and leaves a substantial reserve. The clinical case for dental travel is strongest when the procedure is elective and complex, the cost differential is significant, the receiving clinic operates to verifiable standards, and local aftercare can be arranged.
The decision to travel for dental rehabilitation is a clinical trust decision, not primarily a financial one. The cost differential justifies the travel only if the clinical outcome is equivalent, and that equivalence is verifiable. The questions worth asking are: Does this clinic operate to the same diagnostic standard as a Canadian specialist? Are the implant systems and prosthetic materials the same? Is the warranty a documented contract with specific terms, or is it promotional language? Is there a 10-year open file, or does the clinical relationship end at the airport?
At Stunning Dentistry, we do not create a timeline pressure for the treatment decision. The remote pre-assessment is provided without obligation. The diagnostic appointment is the commitment point, and that commitment is to a clinical evaluation, not a treatment contract. No irreversible procedure begins without the three-stage patient approval gate being completed and documented.
| Factor | Favours Travelling | Favours Treating Locally |
|---|---|---|
| Cost differential | ≥CAD $30,000 saving | Marginal, travel cost absorbs the saving |
| Procedure complexity | High; interdisciplinary team required | Low; single-unit; manageable locally |
| Clinic verification | Credentials and protocols verifiable | Cannot verify receiving clinic standards |
| Medical profile | Stable; cleared for travel post-surgery | Active systemic condition requiring local monitoring |
| Local aftercare | Canadian dentist willing to provide maintenance | No local dental support available |
| Urgency | Elective; time to plan and travel | Emergency or acute; needs immediate local management |
Ready to discuss your options?
Pre-Travel Checklist for Canadian Patients
Clinical preparation
- [ ] Existing dental records and X-rays submitted and remote pre-assessment received
- [ ] Preliminary modality and CAD cost range confirmed in writing
- [ ] GP liaison completed if diabetes, bisphosphonate use, anticoagulant therapy, or recent jaw radiotherapy
- [ ] Current medication list prepared (generic and brand names, doses)
- [ ] Allergy history documented (including anaesthetic allergies if known)
- [ ] Flights booked: direct or single-connection route recommended
- [ ] Accommodation confirmed within reasonable distance of Stunning Dentistry
- [ ] Travel insurance confirmed: pre-existing condition coverage; medical evacuation coverage
- [ ] Extended health benefits policy reviewed: implant coverage terms for treatment abroad confirmed
Post-treatment preparation
- [ ] Canadian dentist briefed: willing to provide 6-monthly hygiene maintenance and annual radiographic review
- [ ] Soft diet period understood: 3–4 months post-surgery for full-arch implant cases
- [ ] Night guard discussed: fitted in India or arranged locally on return
- [ ] Emergency contact protocol confirmed with Stunning Dentistry before travel
- [ ] Return-visit timing discussed for definitive phase if implant case
Curious about costs and timelines?
Book a Clinical Evaluation
If you are uncertain whether full-mouth rehabilitation is indicated for your case, the appropriate next step is a diagnostic evaluation, not a treatment commitment.
Secondary CTA: Request Remote Case Review
Want a personalised treatment plan?
Questions about this procedure?

Clinical References
1. Maló P, et al. "All-on-4 immediate-function concept for completely edentulous maxillae: a clinical report on the medium (3 years) and long-term (5 years) outcomes." *Clinical Oral Implants Research.* 2012.
"name": "Prosthodontics"
Ready to discuss your options?
Specialist-only treatment planning
- Remote file review before travel
- Evidence-led treatment checkpoints
No waiting list for eligible cases
- Remote file review before travel
- Evidence-led treatment checkpoints
Trip coordinated with care timeline
- Remote file review before travel
- Evidence-led treatment checkpoints
Our Partners











Why Us
Frequently Asked Questions
Is full-mouth rehabilitation permanent?
The implants, when maintained correctly, have documented 15–20-year survival in peer-reviewed cohort data. The prosthetic components, zirconia or ceramic crowns, implant-retained bridges, have documented 10–15-year survival under normal function and maintenance. "Permanent" as an unqualified claim is not accurate for any dental restoration. "Highly durable with documented longevity" is accurate.
Will I be without teeth at any point?
In full-arch implant cases, a full-arch provisional prosthetic is seated on the day of surgery, the patient does not leave without teeth. In tooth-supported cases, temporary crowns are placed at the preparation appointment. There is no edentulous period.
Can I eat normally during the provisional phase?
Within 7–10 days post-surgery, most patients are eating soft foods normally. The soft diet restriction, avoiding hard, crunchy, or tough foods, applies for the first 3–4 months while osseointegration is occurring. After the definitive prosthetic is seated, normal dietary function is restored.
What is the risk of implant rejection?
Implants do not trigger an immune rejection response in the same way as organ transplants, titanium is biologically inert. What occurs instead is failure to osseointegrate, which is driven by bacterial contamination, poor bone quality, insufficient primary stability, or systemic factors (smoking, uncontrolled diabetes). The incidence in well-selected cases is 1–5% at 5 years in the peer-reviewed literature.
Does Stunning Dentistry coordinate with my Canadian dentist?
Yes. Stunning Dentistry provides a clinical summary at discharge that is designed for handover to the Canadian dental team. Remote consultation is available between review appointments. If a local Canadian dentist needs implant-specific information, torque values, implant system details, hygiene protocol, Stunning Dentistry provides it directly.
See your new smile instantly!
This tool will help you understand potential structural and aesthetic changes before finalizing treatment decisions.










